Cystic Acne: The Most Severe Form of Acne — Causes, Treatment, and What to Expect
Medically reviewed by Dr. Sarah Mitchell, MD, Board-Certified Dermatologist
Written by Teen Acne Solutions Editorial Team — Updated March 12, 2026
Key takeaways
- Cystic acne involves large (often >1cm), painful, fluid-filled lesions deep in the dermis
- It has the highest risk of permanent scarring of any acne type — early professional treatment is essential
- Genetics play a major role — if your parents had cystic acne, your risk is significantly higher
- Isotretinoin (Accutane) remains the most effective treatment, with 85% of patients achieving long-term clearance
- No over-the-counter product can effectively treat true cystic acne — see a dermatologist immediately
If you've ever felt a deep, throbbing lump forming under your skin — one that hurts before you can even see it, one that no amount of washing or spot treatment can touch — you may be dealing with cystic acne. It is the most severe form of acne vulgaris, and for the millions of teenagers who experience it, it can feel absolutely devastating.
But here is what you need to know right now, before we go any further: cystic acne is treatable. It requires professional medical intervention, it takes patience, and the journey is not always easy. But the vast majority of people with cystic acne can achieve clear or nearly clear skin with the right approach. This article will walk you through everything — what cystic acne actually is, why it happens, why it hurts so much, and every treatment option available to you today.
What Is Cystic Acne?
Cystic acne is classified as Grade IV (severe nodulocystic) acne under dermatological grading systems. Unlike the whiteheads, blackheads, and surface-level pimples that most teens experience, cystic acne involves large, fluid-filled lesions that form deep within the dermis — the thick middle layer of your skin.
A true acne cyst is typically larger than 1 centimeter in diameter (sometimes much larger), filled with a mixture of pus, dead skin cells, bacteria, and inflammatory fluid. These lesions do not have a visible "head" on the surface of the skin. They sit far below the epidermis, which is why no amount of squeezing, popping, or surface-level treatment can reach them.
Cystic acne most commonly appears on the:
- Face (jawline, cheeks, forehead, and chin)
- Back (sometimes called "bacne")
- Chest
- Shoulders and upper arms
- Neck
It affects roughly 2 to 3 percent of the population at some point, but among teenagers with acne, rates of severe cystic presentations are notably higher — particularly in males between the ages of 15 and 19, when androgen levels surge during puberty.
How Cysts Form: The Biology Behind the Breakout
To understand why cystic acne is so different from regular acne, you need to understand what is happening beneath your skin at a structural level.
All acne begins the same way: a hair follicle (pore) becomes clogged with a combination of excess sebum (oil), dead skin cells, and bacteria — particularly Cutibacterium acnes (formerly Propionibacterium acnes). In mild acne, this blockage stays relatively close to the surface, producing a whitehead or blackhead. In moderate acne, bacteria multiply within the clogged pore, triggering an immune response that creates the red, swollen papules and pustules most people recognize as "pimples."
When the Follicle Wall Ruptures
Cystic acne takes this process dramatically further. The buildup of pressure inside the clogged follicle becomes so intense that the follicle wall ruptures deep within the dermis. When this happens, the mixture of bacteria, sebum, dead cells, and inflammatory chemicals spills out into the surrounding dermal tissue.
Your immune system responds aggressively. White blood cells flood the area, inflammatory cytokines are released in massive quantities, and the body essentially walls off the infection by forming a membrane-bound sac — the cyst. This sac fills with fluid as the inflammatory battle rages, creating that distinctive large, swollen, painful lump.
The Role of Inflammation
Research published in the Journal of Clinical and Aesthetic Dermatology has demonstrated that inflammation in cystic acne is not just a response to bacteria — it is a self-perpetuating cycle. The inflammatory mediators released during the immune response actually damage surrounding tissue, which triggers more inflammation, which causes more tissue damage. This is why cystic lesions can persist for weeks or even months without resolving, and why they cause so much more destruction than surface-level acne.
The body's own immune response, in trying to fight the infection, ends up doing significant collateral damage to the healthy dermal tissue, collagen, and subcutaneous structures around the cyst. This is the fundamental reason cystic acne scars so severely.
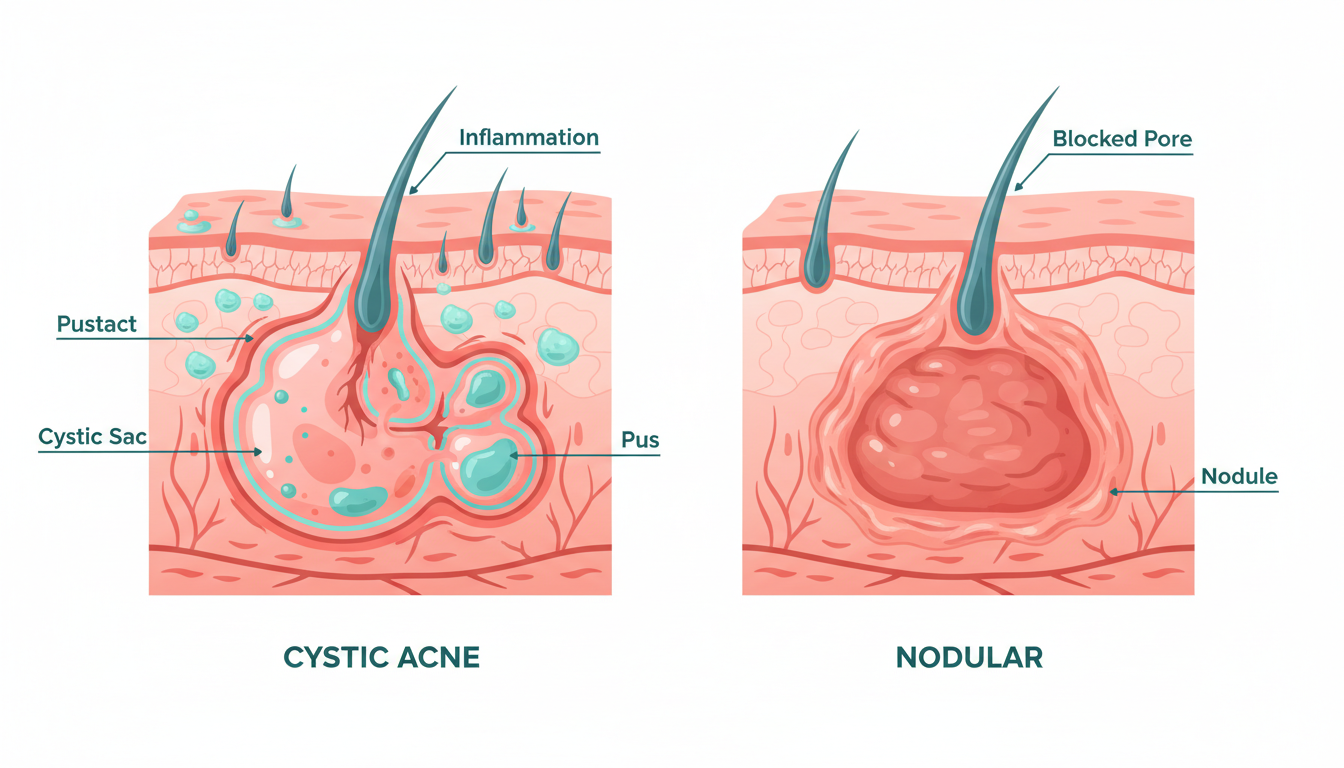
Cystic vs. Nodular Acne: Understanding the Difference
The terms "cystic" and "nodular" are often used interchangeably, but they describe distinct types of severe acne lesions.
Nodular acne involves hard, solid, painful lumps that form deep in the skin. Nodules are firm to the touch, do not contain fluid, and are typically 1 to 2 centimeters in diameter. They result from deep inflammation but without the formation of a fluid-filled sac.
Cystic acne involves softer, fluid-filled lesions. When you press on a cyst (which you should avoid doing), it may feel slightly movable or fluctuant. The fluid inside is a combination of pus, liquefied tissue debris, and inflammatory exudate.
In practice, many people with severe acne have both nodules and cysts simultaneously — a condition dermatologists refer to as nodulocystic acne. The treatment approach is similar for both, but true cysts carry a somewhat higher risk of scarring because the fluid-filled cavity creates a larger area of tissue destruction.
| Feature | Cystic Acne | Nodular Acne |
|---|---|---|
| Texture | Soft, fluid-filled | Hard, solid |
| Size | Often >1 cm, can reach 2-3 cm | Typically 1-2 cm |
| Depth | Deep dermis / subcutaneous | Deep dermis |
| Duration | Weeks to months | Weeks to months |
| Scarring risk | Very high | High |
| Pain level | Severe | Moderate to severe |
Why Is Cystic Acne So Painful?
If you have cystic acne, you already know that the pain is one of the worst parts. Unlike a surface pimple that stings when you touch it, a cyst can throb and ache constantly — sometimes badly enough to interfere with sleep, concentration, and daily life.
There are several reasons for this:
Pressure on Nerve Endings
The dermis is richly supplied with nerve endings, particularly pain receptors (nociceptors). As a cyst expands with fluid, it exerts direct mechanical pressure on these nerve endings. The deeper the lesion, the more nerves it can compress. A large cyst on the jawline, for example, can put pressure on nerve branches that radiate pain across the entire lower face.
Inflammatory Chemical Irritation
The inflammatory mediators released during the immune response — including prostaglandins, bradykinin, and histamine — are potent pain-inducing chemicals. They sensitize the surrounding nerve endings, lowering their pain threshold. This is why even lightly touching the area around a cyst can produce sharp, disproportionate pain.
Tissue Swelling
The massive inflammatory response causes significant swelling in the surrounding tissue. This swelling further compresses nerve endings and restricts blood flow, creating a sustained, aching pain that can persist for the entire lifespan of the lesion.
The Genetic Component: Why Some Teens Get Cystic Acne and Others Don't
One of the most frustrating aspects of cystic acne is how arbitrary it can feel. Two teenagers can eat the same foods, use the same skincare products, have similar hygiene routines, and yet one develops severe cystic acne while the other has perfectly clear skin.
The answer, overwhelmingly, is genetics.
Studies have consistently shown that if one or both of your parents experienced severe acne, your risk of developing cystic acne is significantly higher — some estimates suggest three to four times the baseline risk. The genetic factors influence multiple aspects of acne development:
- Sebum production rates — genetically determined oil production levels
- Follicular keratinization patterns — how quickly dead skin cells shed (or don't) inside your pores
- Inflammatory response intensity — how aggressively your immune system reacts to blocked pores
- Androgen sensitivity — how strongly your skin responds to hormones like testosterone and DHT
- Skin microbiome composition — the baseline bacterial populations on your skin
This is critically important to understand because it means cystic acne is not caused by poor hygiene, eating chocolate, or not washing your face enough. These are persistent myths that cause immense guilt and shame in teenagers who are already suffering. Cystic acne is a medical condition with a strong genetic basis, and it deserves medical treatment — not blame.

Why Over-the-Counter Products Cannot Treat Cystic Acne
Walk into any drugstore and you will find an entire aisle of acne products promising clear skin. Benzoyl peroxide washes, salicylic acid pads, tea tree oil serums, charcoal masks — the list is endless. For mild to moderate acne, some of these products can genuinely help.
For cystic acne, none of them will work.
The reason is simple physics and biology. Over-the-counter acne products are designed to work on the surface of the skin or within the upper layers of the epidermis. A cystic lesion sits deep in the dermis, centimeters below where any topical product can penetrate. No cleanser, toner, mask, or spot treatment can reach the site of a cyst.
Worse, some popular at-home approaches can actually make cystic acne more severe:
- Aggressive scrubbing damages the skin barrier and increases inflammation
- Attempting to pop or squeeze cysts can rupture the cyst membrane deeper into the tissue, spreading the infection and dramatically increasing scarring risk
- Overusing drying products strips the skin, triggering compensatory oil production that feeds more breakouts
If you suspect you have cystic acne, the single most important thing you can do is see a dermatologist as soon as possible. Every week of delay increases the risk of permanent scarring.
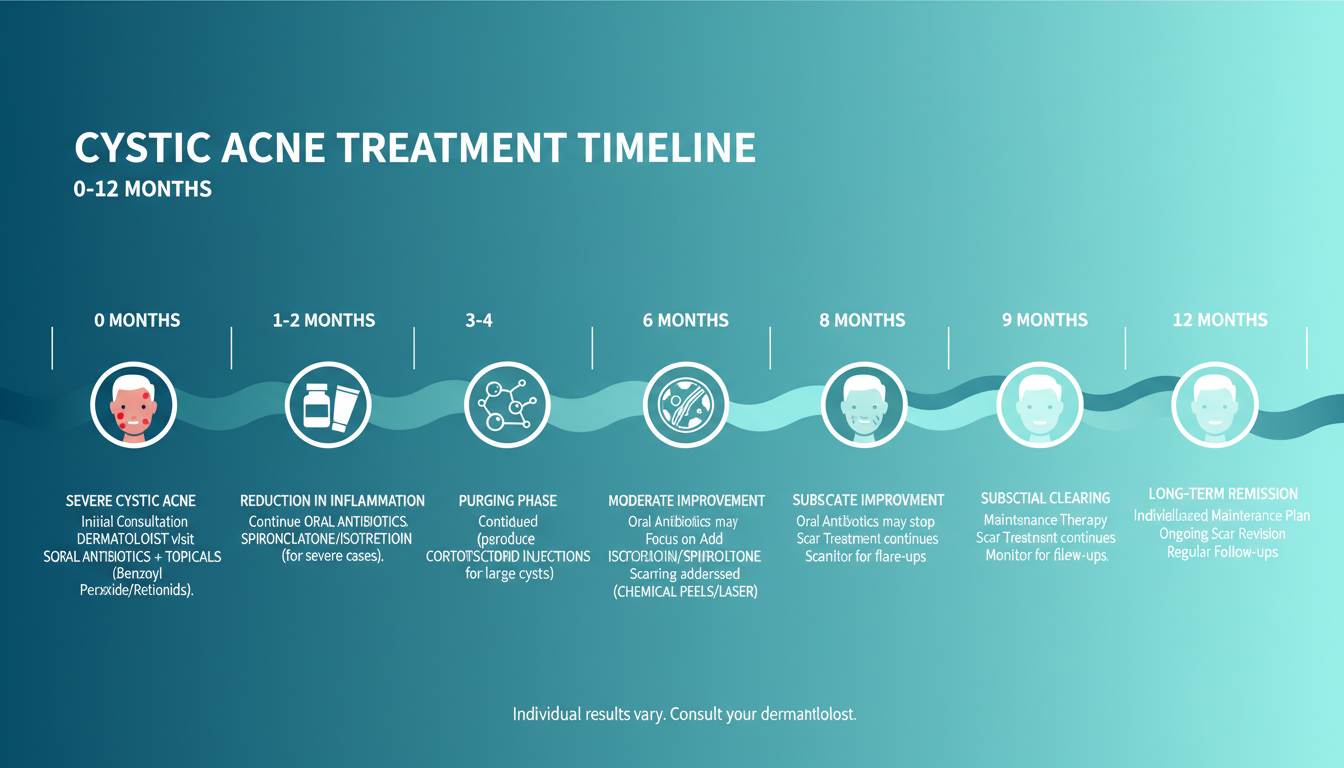
Treatment Options: The Dermatological Ladder for Cystic Acne
Dermatologists approach cystic acne treatment systematically, typically working through a progression of increasingly powerful interventions. The 2016 American Academy of Dermatology guidelines provide a clear framework for how severe acne should be managed.
Step 1: Topical Retinoids as a Baseline
Nearly every cystic acne treatment plan begins with a prescription-strength topical retinoid — tretinoin (Retin-A), adapalene (Differin at prescription strength), or tazarotene (Tazorac). Retinoids work by accelerating skin cell turnover, preventing the clogging that initiates acne formation.
On their own, topical retinoids are not sufficient to control cystic acne. However, they serve as an important foundation that makes other treatments more effective and helps prevent new lesions from forming. Most dermatologists will keep patients on a retinoid throughout the entire treatment process and often as long-term maintenance therapy.
Step 2: Oral Antibiotics
For active cystic breakouts, dermatologists typically prescribe oral antibiotics — most commonly doxycycline or minocycline. These work through two mechanisms: they directly reduce C. acnes bacterial populations and, importantly, they have anti-inflammatory properties that help calm the intense immune response driving cyst formation.
Oral antibiotics usually begin working within 4 to 6 weeks, with peak effects at around 3 months. However, they have significant limitations:
- Antibiotic resistance — long-term use (beyond 3-4 months) is discouraged due to bacterial resistance concerns
- They are not a cure — most patients relapse when antibiotics are stopped
- Side effects — photosensitivity, gastrointestinal upset, and (rarely) more serious complications
Antibiotics are best understood as a bridge therapy — they help control active disease while a more definitive treatment plan is established.
Step 3: Hormonal Therapy (for Females)
For girls and young women whose cystic acne is driven by hormonal fluctuations — particularly acne that flares around menstrual periods and concentrates on the lower face and jawline — hormonal therapy can be remarkably effective.
Options include:
- Combined oral contraceptives — several formulations are FDA-approved specifically for acne, including those containing drospirenone or norgestimate
- Spironolactone — an androgen blocker that reduces the hormonal stimulation of oil glands, typically prescribed at 50-200 mg daily
Hormonal therapy can take 3 to 6 months to show full effects but can produce dramatic and sustained improvement in hormone-driven cystic acne. It is not appropriate for male patients due to its anti-androgen effects.
Step 4: Cortisone Injections for Emergencies
When a large, painful cyst needs rapid treatment — say, before an important event, or when a cyst is so large it risks significant scarring — dermatologists can inject a dilute corticosteroid solution (typically triamcinolone acetonide) directly into the lesion.
Intralesional cortisone injections work remarkably fast. The inflammation and swelling begin to subside within 24 to 48 hours, and the cyst typically flattens significantly within a few days. This is the single fastest treatment for an individual cystic lesion.
However, cortisone shots are a management tool, not a cure. They treat individual cysts but do nothing to prevent new ones from forming. Overuse can also cause localized skin thinning or depressed scars at the injection site.
Step 5: Isotretinoin — The Definitive Treatment
For severe cystic acne that does not respond adequately to other treatments — or for any cystic acne that poses a significant scarring risk — isotretinoin (formerly sold as Accutane) is the gold standard treatment. It is the only medication that addresses all four pathogenic factors of acne simultaneously, and it remains the most effective treatment available for severe cystic acne.
Isotretinoin: What You Need to Know
Isotretinoin deserves its own detailed section because for many teens with cystic acne, it is the treatment that will finally give them clear skin. It is also surrounded by significant fear, misinformation, and legitimate medical considerations that require honest discussion.
How Isotretinoin Works
Isotretinoin is a synthetic form of vitamin A that works through four distinct mechanisms:
- Dramatically reduces sebum production — by up to 90%, by shrinking the sebaceous (oil) glands
- Normalizes follicular keratinization — prevents the dead skin cell buildup that clogs pores
- Reduces C. acnes populations — by eliminating the oily environment bacteria need to thrive
- Has direct anti-inflammatory effects — calming the immune overreaction that drives cyst formation
No other single medication targets all four acne pathways. This is why isotretinoin is so extraordinarily effective.
Success Rates
The numbers speak for themselves. Research published in Dermato-Endocrinology reports that approximately 85 percent of patients achieve complete or near-complete clearance after a single course of isotretinoin. Of those who do relapse, most respond to a second course. Long-term cure rates after one or two courses approach 90 to 95 percent.
For a condition as severe and scarring as cystic acne, these are remarkable outcomes.
Treatment Duration and Dosing
A typical course of isotretinoin lasts 5 to 7 months, though this varies based on the patient's weight, the severity of their acne, and how they tolerate the medication. The standard cumulative dose target is 120-150 mg per kilogram of body weight over the entire course.
Most patients begin at a lower dose that is gradually increased. It is common to experience an initial flare (temporary worsening) in the first 2 to 4 weeks as the skin purges. This can be discouraging, but it is a normal and expected part of the process.
Significant improvement usually becomes visible by month 2 to 3, with continued improvement throughout the course. Many dermatologists continue treatment for 1 to 2 months after the skin has fully cleared to reduce relapse risk.
Side Effects: An Honest Discussion
Isotretinoin has a well-documented side effect profile, and you deserve honest information about what to expect.
Common side effects (experienced by most patients):
- Dry skin and lips — this is nearly universal and often severe. Quality lip balm and moisturizer become essential
- Dry eyes — contact lens wearers may need to switch to glasses temporarily
- Dry nasal passages — nosebleeds are common, especially in dry climates
- Muscle and joint aches — particularly during physical activity
- Sun sensitivity — strict sun protection is mandatory
- Elevated blood lipids — regular blood monitoring is required
Less common but important side effects:
- Headaches — usually mild, but severe persistent headaches should be reported immediately
- Mood changes — the relationship between isotretinoin and depression has been extensively studied (discussed below)
- Night vision changes — temporary in most cases
- Hair thinning — usually temporary and reverses after treatment
The depression question: The potential link between isotretinoin and depression or suicidal ideation has been one of the most studied and debated topics in dermatology. Large-scale epidemiological studies have produced mixed results — some show a slight increase in depression risk, while others show that clearing severe acne actually improves mental health. The current medical consensus, as reflected in AAD guidelines, is that isotretinoin can be safely prescribed with appropriate mental health monitoring. Your dermatologist will screen for depression before and during treatment, and any mood changes should be reported immediately.
The critical absolute contraindication: Isotretinoin causes severe birth defects and must never be taken during pregnancy. Female patients of childbearing potential must participate in the iPLEDGE program (in the United States), which requires two forms of contraception and monthly pregnancy tests throughout treatment and for one month after stopping.
The iPLEDGE Program
For female patients in the U.S., the iPLEDGE program is a mandatory registration system designed to prevent isotretinoin-exposed pregnancies. It requires:
- Registration in the iPLEDGE system before starting treatment
- Monthly pregnancy tests (two negative tests before starting, then monthly)
- Two simultaneous forms of contraception (or documented abstinence)
- Monthly check-ins with the iPLEDGE system to receive each prescription
- A 7-day prescription window — if you do not pick up your prescription within 7 days, you must get a new pregnancy test
The iPLEDGE requirements can feel burdensome, but they exist for an important medical reason. Your dermatologist's office will help you navigate the system.
Scarring and Recovery: What Cystic Acne Leaves Behind
One of the most urgent reasons to seek early treatment for cystic acne is its extremely high risk of permanent scarring. The deep tissue destruction caused by cystic lesions damages the collagen structure of the dermis, and this damage often does not fully heal on its own.
Types of Acne Scars
Cystic acne can produce several types of scars:
- Ice pick scars — narrow, deep, pitted scars that extend into the deep dermis. These are the most difficult to treat
- Boxcar scars — wider, rectangular depressions with sharply defined edges
- Rolling scars — broad, shallow undulations caused by fibrous bands tethering the skin to deeper structures
- Hypertrophic or keloid scars — raised, thickened scar tissue, more common on the chest, back, and jawline
- Post-inflammatory hyperpigmentation — dark marks left after a cyst heals. Technically not scars, these usually fade over months to years but can be persistent in darker skin tones
Scar Treatment Options
Once active cystic acne is fully controlled, a range of treatments can significantly improve scarring:
- Microneedling — stimulates collagen remodeling through controlled micro-injuries
- Fractional laser resurfacing — ablative (CO2, erbium) and non-ablative options can dramatically improve scar texture
- Chemical peels — medium and deep peels can improve shallow scarring
- Dermal fillers — can temporarily elevate depressed scars
- Subcision — a minor procedure that releases fibrous bands beneath rolling scars
- TCA cross — trichloroacetic acid applied directly into ice pick scars to stimulate filling from below
Most patients benefit from a combination approach tailored to their specific scar types. Scar revision is an ongoing area of medical advancement, and newer techniques continue to improve outcomes. However, prevention through early treatment remains far more effective than treating scars after they form.
The Emotional Impact: Why Cystic Acne Is More Than Skin Deep
We need to talk about something that medical articles too often gloss over: the emotional and psychological devastation that cystic acne causes.
A 2011 study published in the Journal of Investigative Dermatology found that adolescents with acne had significantly higher rates of depressive symptoms and suicidal ideation compared to their clear-skinned peers. The association was dose-dependent — the more severe the acne, the greater the psychological impact. Cystic acne, as the most severe form, carries the heaviest emotional burden.
What Teens With Cystic Acne Often Experience
- Social withdrawal — avoiding friends, skipping events, not wanting to leave the house
- Obsessive mirror-checking or conversely, avoiding mirrors entirely
- Declining academic performance — difficulty concentrating when in pain or distressed about appearance
- Depression and anxiety — clinical levels that may require separate treatment
- Anger and frustration — especially when well-meaning people offer unhelpful advice like "just wash your face" or "stop eating junk food"
- Body dysmorphia — perceiving their skin as far worse than others see it
- Loss of self-confidence during critical developmental years
If you are experiencing any of these feelings, please know: your pain is valid, your feelings are normal, and you are not alone. Cystic acne is not a cosmetic inconvenience — it is a medical condition that causes real physical pain and real emotional suffering. You deserve compassionate, effective treatment.
When to Seek Mental Health Support
If cystic acne is significantly affecting your mood, your relationships, your school performance, or your desire to participate in life, talk to someone. This could be a parent, a school counselor, your dermatologist, or a mental health professional. There is no weakness in asking for help — there is only wisdom.
Many dermatology practices now routinely screen for depression and anxiety in their acne patients, reflecting the medical community's growing recognition that treating the skin and treating the mind are inseparable when it comes to severe acne.
When to Push for Aggressive Treatment
Too many teens with cystic acne spend months or even years cycling through ineffective treatments before being referred for isotretinoin or other aggressive therapy. During that time, their skin is scarring irreversibly.
You should advocate for aggressive treatment if:
- You have multiple cystic lesions that are not responding to topical treatment and oral antibiotics after 3 months
- Your acne is actively scarring — you can see pitted or depressed marks forming
- Your acne is severely impacting your mental health or quality of life
- You have a strong family history of severe, scarring acne
- Your cysts are very large (>2 cm), very painful, or producing sinus tracts (tunnels between cysts)
You have the right to ask your dermatologist about isotretinoin or to request a referral to a dermatologist who prescribes it. If your current provider is reluctant to escalate treatment while your skin is scarring, seek a second opinion. This is your face, your body, and your future. Early, aggressive treatment for severe cystic acne is not an overreaction — it is the medically appropriate response.

There Is Real Hope: You Will Get Through This
If you are reading this article because you are currently living with cystic acne, we want to end on the most important point: this condition is temporary and treatable.
The statistics bear this out. With isotretinoin, 85 percent of patients achieve lasting clearance. With combination approaches, the numbers are even higher. The treatments available today are more effective, better understood, and more accessible than at any point in medical history.
Thousands of adults who once had severe cystic acne now have clear, healthy skin. Many of them will tell you that the journey was difficult — the initial flares, the dry skin, the blood tests, the monthly dermatology appointments — but that reaching the other side was worth every moment of it.
Your cystic acne does not define you. It is not a reflection of your hygiene, your character, or your worth. It is a medical condition driven largely by genetics and hormones, and it responds to medical treatment.
Take the first step. Talk to a dermatologist. Bring this article if it helps. Advocate for yourself. And know that clearer skin — and the confidence that comes with it — is not just a possibility. For the vast majority of people with cystic acne, it is an inevitability.
You just need the right treatment, the right doctor, and the patience to see it through.
This article was medically reviewed by Dr. Sarah Mitchell, MD, a board-certified dermatologist specializing in adolescent acne treatment. It is intended for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment of cystic acne.
How we reviewed this article:
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
- Zaenglein AL, et al. (2016). Guidelines of care for the management of acne vulgaris. JAAD.https://pubmed.ncbi.nlm.nih.gov/26897386/
- Strauss JS, et al. (2007). Guidelines of care for acne vulgaris management. JAAD.https://pubmed.ncbi.nlm.nih.gov/17276540/
- Layton AM. (2009). The use of isotretinoin in acne. Dermato-Endocrinology.https://pubmed.ncbi.nlm.nih.gov/20436870/
- Kraft J, Freiman A. (2011). Management of acne. CMAJ.https://pubmed.ncbi.nlm.nih.gov/21398228/
- Bhate K, Williams HC. (2013). Epidemiology of acne vulgaris. British Journal of Dermatology.https://pubmed.ncbi.nlm.nih.gov/23210645/
- Gollnick H, et al. (2003). Management of acne. JAAD.https://pubmed.ncbi.nlm.nih.gov/12734496/
- Tanghetti EA. (2013). The role of inflammation in acne pathology. JCAD.https://pubmed.ncbi.nlm.nih.gov/24062871/
- Halvorsen JA, et al. (2011). Suicidal ideation and mental health in adolescents with acne. JID.https://pubmed.ncbi.nlm.nih.gov/20944653/
- American Academy of Dermatology. Severe acne: Types and treatments.https://www.aad.org/public/diseases/acne/really-acne/severe
- Dréno B, et al. (2015). Understanding innate immunity and inflammation in acne. JEADV.https://pubmed.ncbi.nlm.nih.gov/25382740/
- Thiboutot DM, et al. (2009). New insights into acne management. JAAD.https://pubmed.ncbi.nlm.nih.gov/19467365/
Read This Next

Acne Face Mapping: Does Where You Break Out Tell You Why?

PCOS and Acne in Teens: When Breakouts Signal Something Bigger
If your acne won't respond to normal treatments and comes with irregular periods, it might be PCOS. Here's what teen girls and their parents need to know about diagnosis and treatment.
Read More →
Testosterone and Acne: Why Hormones Drive Most Teen Breakouts
Testosterone gets converted to DHT, which ramps up your oil glands. This is the core reason acne peaks during puberty and why boys tend to get it worse than girls.
Read More →
Inflammatory Acne: Papules, Pustules, and Why Your Skin Hurts
Inflammatory acne is the red, painful kind that actually hurts. Understanding the immune response behind it changes how you treat it and helps you stop making it worse.
Read More →
Comedonal Acne: Why Your Skin Is Bumpy But Not Red (And How to Fix It)
Comedonal acne gives you textured, bumpy skin without the redness of typical pimples. It's frustrating because it doesn't respond to the usual treatments. Here's what actually works.
Read More →