Pustules: The Classic Pimple — What's Inside, Should You Pop It, and How to Treat It
Medically reviewed by Dr. James Chen, MD, Dermatology & Nutrition
Written by Teen Acne Solutions Editorial Team — Updated March 14, 2026
Key takeaways
- The white/yellow center of a pustule is pus — a mixture of dead white blood cells, bacteria, and skin debris
- Popping pustules at home risks pushing bacteria deeper, causing worse infection and scarring
- Spot treatments with benzoyl peroxide (2.5-5%) are the most effective way to shrink a pustule quickly
- Hydrocolloid pimple patches can safely draw out fluid and protect the area from picking
- If you're getting more than a few pustules regularly, it's time to see a dermatologist
When someone says "I have a pimple," they are almost always talking about a pustule — the red, slightly swollen bump with a white or yellowish head sitting right at the center. It seems to appear overnight, always right before something important. School photo day. A first date. A presentation.
But as common as pustules are, most people do not understand what is actually happening inside them. That white center is not just "gunk" — it is the visible evidence of your immune system fighting a battle beneath your skin. And what you do next can make the difference between a blemish that fades in days and a mark that lingers for months.
What Are Pustules
A pustule is an inflamed acne lesion — a raised, red bump with a visible collection of pus at or near the surface. In dermatology, pustules are classified as a type of inflammatory acne, which means the immune system is actively involved in creating the blemish. This sets them apart from non-inflammatory acne like blackheads and whiteheads, which are just clogged pores without a significant immune response.
Pustules are what most people mean when they use the word "pimple." They typically range from a few millimeters to about a centimeter in diameter, and the hallmark feature is that visible white or yellow center — called the pustular head — surrounded by a ring of redness and mild swelling.
Where Do Pustules Show Up?
For teenagers, the most common locations are:
- The face — especially the forehead, nose, chin, and cheeks (the T-zone is a particular hotspot)
- The upper back and shoulders — areas dense with oil glands
- The chest — another zone where sebaceous glands are concentrated
Pustules can appear as isolated spots or in clusters, often alongside other acne types like blackheads, whiteheads, and papules.
What's Inside a Pustule
This is the question everyone asks, usually while staring at a mirror: what is that stuff?
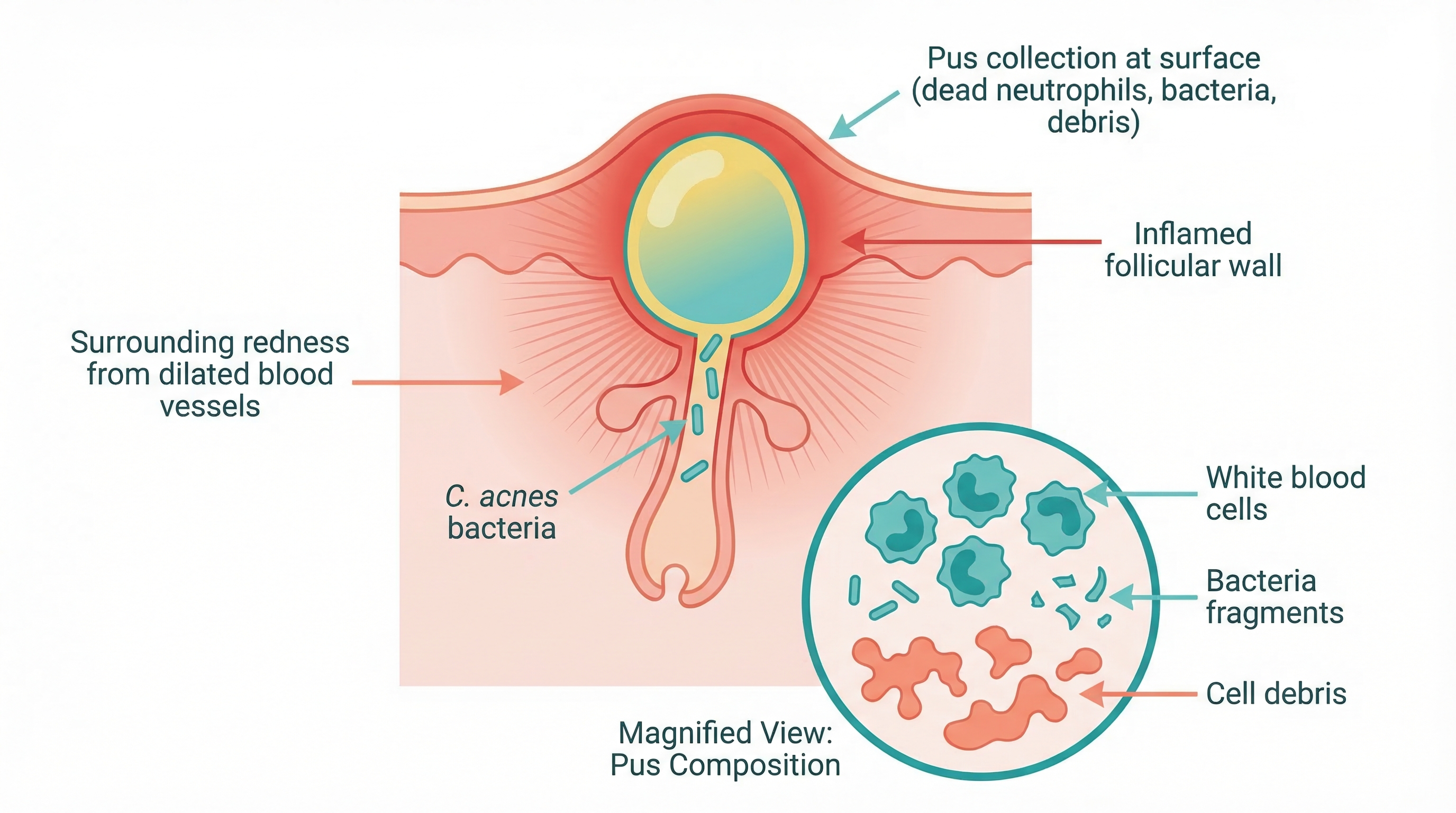
The white or yellowish material at the center of a pustule is pus. And despite how it looks, pus is not just dirt or oil. It is the aftermath of an immune response. Here is what it is made of:
- Dead neutrophils (white blood cells): When bacteria multiply inside a clogged pore, your immune system sends neutrophils — a type of white blood cell — to the site to fight the infection. These cells attack bacteria and then die, accumulating in the area. Dead neutrophils are the primary component of pus and what gives it that white-to-yellowish color.
- Bacteria and bacterial debris: The bacterium most associated with acne is Cutibacterium acnes (C. acnes), which lives naturally on the skin. When a pore becomes clogged and the environment inside becomes low-oxygen, C. acnes can multiply rapidly. The immune response kills many of these bacteria, but their remnants remain in the pus.
- Sebum (oil): The excess oil that helped create the clogged pore in the first place is also mixed in.
- Dead skin cells: Cells that lined the hair follicle and were shed into the pore contribute to the overall mixture.
- Inflammatory molecules: Enzymes and chemical signals released during the immune response — including cytokines and matrix metalloproteinases — are part of the fluid as well.
So when you look at a pustule, you are essentially seeing the visible result of a microscopic battle. Your immune system detected a problem, sent soldiers to fight it, and the casualties from both sides accumulated near the surface. Fresh pus tends to appear white, while older or more concentrated pus shifts toward yellow.
The Life Cycle of a Pimple: From Clogged Pore to Pustule
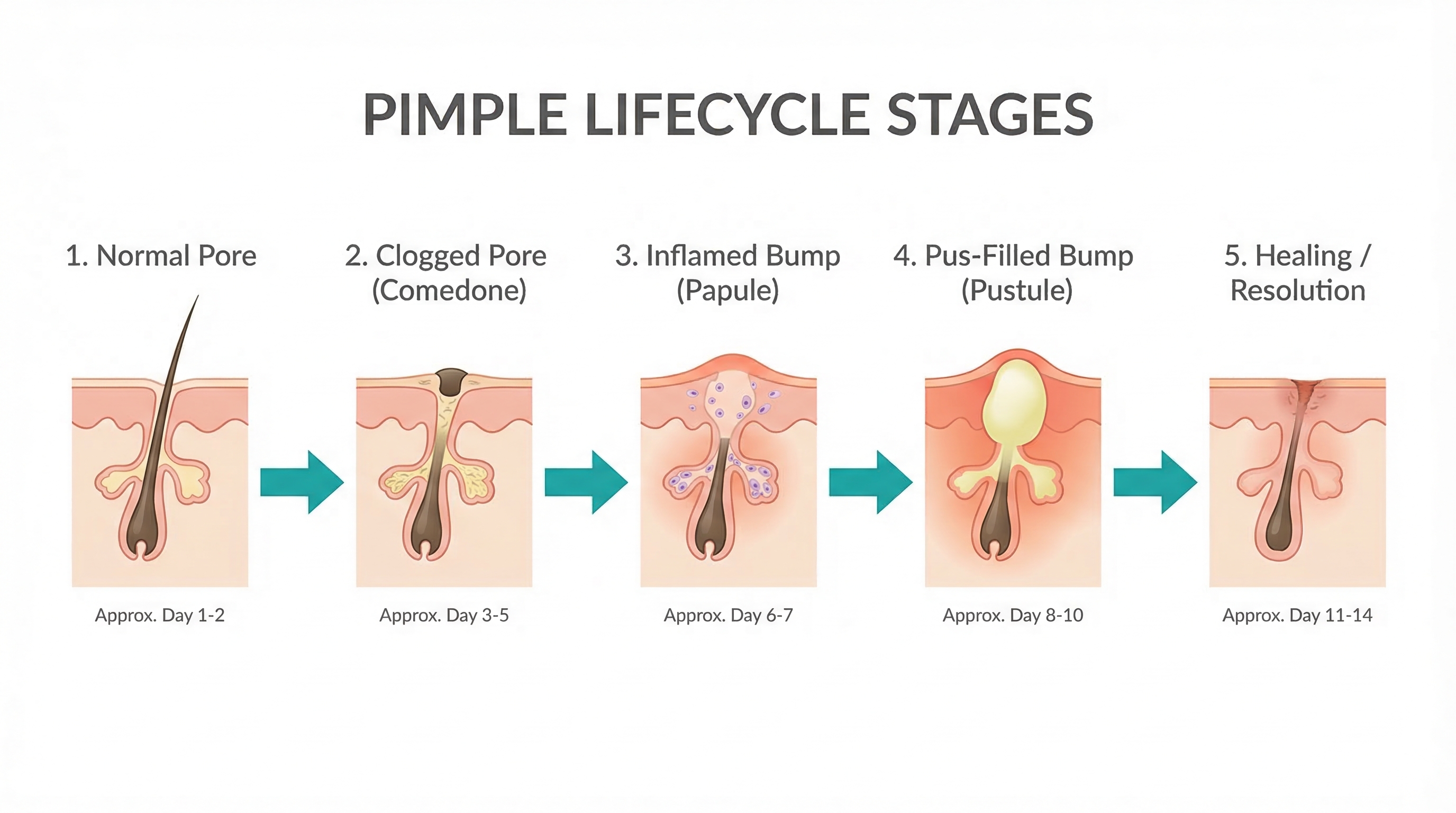
Pustules do not appear out of nowhere, even though it can feel that way. Every pustule follows a progression — a life cycle that typically takes several days to a couple of weeks from start to finish. Understanding this process helps explain why certain treatments work at different stages.
Stage 1: The Microcomedone (Invisible)
Everything starts with a microcomedone — a clogged pore so tiny that you cannot see it with the naked eye. Dead skin cells that normally shed from the lining of the hair follicle become sticky and clump together, trapping sebum inside the pore. Microcomedones can take weeks to develop before anything is visible on the surface, which is why breakouts can feel so unpredictable.
Stage 2: The Comedone (Blackhead or Whitehead)
As the plug grows, the pore becomes visibly blocked. A closed pore produces a whitehead; an open pore allows the material to oxidize and darken, creating a blackhead. At this stage, there is no significant inflammation.
Stage 3: The Papule (Red Bump, No Head)
The clogged environment — low oxygen, rich in oil — becomes a breeding ground for C. acnes bacteria. As they multiply, your immune system mounts a response, sending white blood cells to the area. The result is a papule: a red, tender bump without a visible head. If you have ever felt a sore spot on your face before you could see anything, you were experiencing a papule forming.
Stage 4: The Pustule (The Classic Pimple)
As the immune response continues, dead neutrophils, bacteria, and debris accumulate near the surface, forming the visible white or yellow head that defines a pustule. Not every papule becomes a pustule — some resolve before reaching that stage.
Stage 5: Resolution (or Escalation)
From here, a pustule can go one of two ways. In most cases, the immune system wins — the body reabsorbs the pus, inflammation subsides, and the skin heals within 3 to 7 days (though temporary redness or dark marks may linger). But if the follicle wall ruptures deeper beneath the skin, infected material can spread into surrounding tissue, leading to a nodule or cyst — far more severe lesions with a much higher risk of permanent scarring.
Should You Pop a Pimple
Let's address the question that every teenager (and honestly, every adult) has asked: can I just pop it?
The short answer from dermatologists is no. The American Academy of Dermatology explicitly advises against popping pimples at home, and there are solid medical reasons behind this recommendation.
Why Popping Is Risky
When you squeeze a pustule with your fingers, several things can go wrong:
-
You push bacteria deeper. The pressure you apply does not just push pus outward. It can also force infected material deeper into the dermis — the deeper layer of skin. This can cause a small, surface-level pustule to become a large, deep nodule or cyst. In other words, popping can make the problem significantly worse.
-
You introduce new bacteria. Your fingers, even freshly washed ones, carry bacteria. Squeezing a pustule with unsterilized fingers can introduce additional bacteria into an already compromised area, leading to secondary infection.
-
You damage surrounding tissue. The pressure required to extract a pustule manually can rupture the follicle wall beneath the surface. Once that wall breaks, inflammatory material spreads into surrounding tissue, causing more redness, more swelling, and a longer healing time.
-
You increase the risk of scarring. All of the above — deeper infection, tissue damage, prolonged inflammation — significantly increase the likelihood of permanent scarring. The kind of shallow, pitted scars (atrophic scars) that many adults carry from their teenage years are often the result of picked or squeezed pimples, not the pimples themselves.
-
You create post-inflammatory marks. Even without scarring, aggressive squeezing leads to more intense and longer-lasting hyperpigmentation — dark or red marks that can take weeks or months to fade.
Is There Ever a Safe Way to Pop?
Some dermatologists acknowledge that a truly "ripe" pustule — one where the white head is very close to the surface and looks ready to drain on its own — can be gently expressed with minimal risk if done correctly. But "correctly" is the key word, and it looks nothing like what most people do in front of a mirror.
If a pustule is truly ready to drain, this is the safest approach at home:
- Apply a warm compress for a few minutes to soften the area.
- Wrap clean tissue around each index finger.
- Apply gentle, steady pressure from the sides of the pustule — not from the top — and slightly below the head.
- If it does not drain easily with light pressure, stop. It is not ready.
- Apply an antiseptic or spot treatment afterward.
However, most dermatologists would still tell you that you are better off using a pimple patch or spot treatment and leaving it alone. The risk-to-reward ratio of popping simply is not in your favor.
How Dermatologists Extract Pustules
When a dermatologist extracts a pustule, they use sterilized instruments — typically a comedone extractor — in a controlled environment. They may lance the surface with a sterile needle first, then apply even, targeted pressure to minimize the chance of pushing material deeper. This is why the AAD's advice is straightforward: if a blemish is bothering you enough to want it extracted, see a dermatologist.
How to Treat Pustules
The good news is that pustules are one of the more treatable forms of acne. Because the infection is relatively close to the surface, topical treatments can be very effective. Here are the options with the strongest evidence behind them.
Benzoyl Peroxide: The Gold Standard Spot Treatment
Benzoyl peroxide (BP) is one of the most studied and recommended over-the-counter acne treatments available, and it is particularly effective against pustules. Here is why:
- It kills C. acnes bacteria. BP is an antimicrobial agent that works by releasing oxygen into the pore. Since C. acnes thrives in low-oxygen environments, this is directly lethal to the bacteria driving the infection.
- Bacteria cannot become resistant to it. Unlike antibiotics, BP kills bacteria through oxidation rather than a biological mechanism that bacteria can adapt to. This means it remains effective long-term.
- It reduces inflammation. By killing the bacteria that trigger the immune response, BP indirectly reduces the redness and swelling of a pustule.
For spot-treating individual pustules, a concentration of 2.5% to 5% is ideal. Research has shown that 2.5% BP is just as effective as higher concentrations (up to 10%) for killing bacteria, while causing significantly less dryness and irritation. Apply a thin layer directly to the pustule once or twice daily.
Important tip: Benzoyl peroxide bleaches fabric. Use white towels and pillowcases, and let the product dry completely before contact with clothing.
Salicylic Acid: Best for Prevention, Decent for Treatment
Salicylic acid (SA) is a beta-hydroxy acid that is oil-soluble, meaning it can penetrate into clogged pores and dissolve the mix of dead skin cells and sebum that formed the plug. It is better at preventing new pustules than treating existing ones, but its mild anti-inflammatory properties can help a developing pustule resolve faster. A 2% salicylic acid cleanser or leave-on treatment is the standard concentration.
SA and BP can be used together — many dermatologists recommend a salicylic acid cleanser combined with a benzoyl peroxide spot treatment — but introducing both at once can cause significant dryness. Start with one and add the other gradually.
Sulfur
Sulfur absorbs excess oil and has mild antibacterial properties, making sulfur-based spot treatments effective for drying out individual pustules. The smell is the main downside, though many modern formulations mask it well.
Tea Tree Oil: The Natural Option
A concentration of 5% tea tree oil has been shown to be comparable in efficacy to 5% benzoyl peroxide for mild-to-moderate acne, though it works more slowly. It is a reasonable natural option, but it should always be diluted properly — never applied at full strength, as it can cause irritation.
Ice for Swelling
This is a simple trick that dermatologists recommend for bringing down the redness and swelling of an inflamed pustule quickly:
- Wrap an ice cube in a clean cloth or paper towel.
- Hold it against the pustule for 1 to 2 minutes at a time, with breaks in between.
- Repeat several times.
Ice constricts blood vessels in the area, reducing redness and swelling temporarily. It will not treat the underlying infection, but if you have a visible pustule before an event, icing can make it noticeably less prominent within 15 to 20 minutes. Follow up with a spot treatment for actual healing.
Pimple Patches — Do They Work
Hydrocolloid pimple patches have become enormously popular in the last several years, especially among teenagers. You may have seen them — small, round, translucent stickers that you place over a pimple, usually before bed. But do they actually do anything, or are they just a marketing trend?
How Hydrocolloid Patches Work
Hydrocolloid is a type of wound-dressing material that has been used in medical settings for decades to help heal wounds like blisters and ulcers. The material contains gel-forming agents that absorb moisture and fluid from the wound surface, creating a moist environment that promotes healing.
When applied to a pustule:
- The patch absorbs fluid. As the pustule drains (which it does naturally over time), the hydrocolloid material draws out pus and excess fluid. You can see this happening — the patch turns white and swollen where it has absorbed material.
- It creates a sealed environment. The patch acts as an occlusive barrier, protecting the area from external bacteria, dirt, and your fingers. This sealed, moist environment also promotes faster healing compared to leaving the area exposed.
- It physically prevents picking. This might be the most underrated benefit. If you are someone who compulsively touches or picks at pimples, a patch creates a physical barrier between your fingers and the blemish. For many teens, this alone makes a meaningful difference in outcomes.
What the Evidence Says
Hydrocolloid dressings have a well-established evidence base for wound healing. Their specific use for acne has less formal trial data, but the mechanism is well understood and dermatologists widely consider them a safe option. Some patches include active ingredients like salicylic acid or niacinamide, but basic hydrocolloid patches without added actives still work well.
When Pimple Patches Work Best
Pimple patches are most effective on:
- Pustules with a visible head — these are the lesions with fluid close to the surface that the patch can actually absorb
- Pimples that have already been (carefully) popped — if you have already drained a pustule, a patch helps the area heal cleanly
They are less effective on:
- Deep nodules or cysts — the fluid is too far below the surface for a hydrocolloid patch to reach
- Papules without a head — there is no surface-level fluid to absorb
- Blackheads and whiteheads — these are non-inflammatory and do not contain pus
How to Use Them
Apply the patch to clean, dry skin — no moisturizer or spot treatment underneath, as these prevent the hydrocolloid from contacting the pustule. Leave it on for at least 6 hours (overnight is ideal) and replace with a fresh one if fully saturated.
When a Pustule Is Actually Something Else
Not every bump with a white center is an acne pustule, and the treatment varies depending on the cause.
- Folliculitis is a hair follicle infection (often bacterial or fungal) that looks like acne but tends to appear in areas of friction or shaving and may itch rather than feel tender.
- Milia are tiny, hard, white keratin cysts beneath the skin — not inflamed, not pus-filled, and unresponsive to acne treatments.
- Cold sores are clusters of fluid-filled blisters near the lips that tingle or burn before appearing, containing clear fluid rather than pus.
- Rosacea pustules look similar to acne but come with persistent facial redness, visible blood vessels, and sensitivity.
If you are unsure whether your bumps are actually acne, a dermatologist can tell the difference quickly.
Preventing Pustules
Treating individual pustules is important, but the real goal is preventing them from forming in the first place. Since you now understand the life cycle — clogged pore to comedone to papule to pustule — prevention means intervening at the earliest stages.
Keep Pores Clear
The foundation of pustule prevention is a consistent skincare routine:
- A gentle, non-comedogenic cleanser used twice daily. Avoid harsh scrubs, which disrupt the skin barrier and can worsen acne.
- A topical retinoid (adapalene 0.1% is available over the counter). Retinoids normalize the way skin cells shed inside the follicle, preventing the clumping that leads to microcomedones. If you only add one product to prevent acne, this is it.
- Non-comedogenic moisturizer and sunscreen. Even acne-prone skin needs moisture — dehydrated skin produces more oil to compensate.
Reduce Bacterial Load
Using a benzoyl peroxide wash (4-5%) as part of your routine — even on clear days — helps keep C. acnes bacteria in check. This is particularly useful for the back and chest, where leave-on products are impractical.
Hands Off Your Face
Simple but difficult: stop touching your face. Your hands transfer bacteria, oil, and dirt every time you rest your chin in your hand or pick at a spot. It is one of the easiest behavioral changes for acne prevention.
Manage Contributing Factors
While diet and lifestyle do not cause acne the way hormones and genetics do, certain factors can make breakouts worse. High-glycemic foods (sugary snacks, white bread, processed carbohydrates) spike insulin levels and can increase oil production. Stress triggers cortisol release, worsening inflammation. And simple environmental factors matter too — change pillowcases at least weekly and clean your phone screen regularly, since both can transfer bacteria to your face.

When to See a Doctor
Many teenagers can manage occasional pustules with over-the-counter treatments and a good skincare routine. But there are clear signs that it is time to involve a dermatologist:
You Are Getting Pustules Regularly
If you are dealing with more than a handful of pustules at any given time, or if new ones appear as fast as old ones heal, over-the-counter products alone are unlikely to get the situation under control. A dermatologist can prescribe stronger topical treatments (like prescription-strength retinoids or topical antibiotics combined with benzoyl peroxide) or oral medications if needed.
Over-the-Counter Products Are Not Working After 8-12 Weeks
Most OTC acne treatments need at least 6 to 8 weeks of consistent use before you can judge their effectiveness. If you have given a product a genuine trial — using it correctly and consistently for 2 to 3 months — and you are not seeing meaningful improvement, that is a clear signal to escalate to professional care.
You Are Developing Nodules or Cysts
If your pustules are being joined by large, deep, painful lumps beneath the skin — nodules or cysts — this is moderate-to-severe acne that typically requires prescription treatment. These deeper lesions carry a significantly higher risk of permanent scarring, so early intervention matters.
You Are Scarring
If pustules are leaving behind indented or raised scars (not just flat red or brown marks, which are temporary), treatment is urgent. A dermatologist can recommend more aggressive treatment to prevent further permanent damage.
Your Acne Is Affecting Your Mental Health
If acne is causing significant anxiety, social withdrawal, or depression, that impact on quality of life is a legitimate reason to seek professional help. You do not need "severe" acne to deserve treatment.
What a Dermatologist Might Prescribe
Prescription options for recurring pustules include topical retinoids (tretinoin, tazarotene) at higher strengths than OTC adapalene, topical antibiotics (clindamycin) combined with benzoyl peroxide, oral antibiotics (doxycycline, minocycline) for moderate cases, hormonal therapies (oral contraceptives, spironolactone) for girls with hormone-driven acne, and isotretinoin (Accutane) for severe, treatment-resistant acne.
The Bottom Line
Pustules are the most common and recognizable form of acne. If you are a teenager dealing with them, you are in the overwhelming majority — nearly 85% of people between ages 12 and 24 experience acne.
Resist the urge to pop. Use evidence-based treatments: benzoyl peroxide for active pustules, retinoids for prevention, and hydrocolloid patches to protect and heal individual spots. Build a consistent, gentle skincare routine. And if over-the-counter options are not cutting it, see a dermatologist — there is no reason to struggle when effective prescription treatments exist.
The pustule on your face is just your immune system doing its job, a little too enthusiastically. With the right approach, you can work with your skin instead of against it.
How we reviewed this article:
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
- Zaenglein AL, et al. (2016). Guidelines of care for the management of acne vulgaris. JAAD.https://pubmed.ncbi.nlm.nih.gov/26897386/
- Tanghetti EA. (2013). The role of inflammation in the pathology of acne. JCAD.https://pubmed.ncbi.nlm.nih.gov/24062871/
- Dréno B, et al. (2015). Understanding innate immunity and inflammation in acne. JEADV.https://pubmed.ncbi.nlm.nih.gov/25382740/
- Kraft J, Freiman A. (2011). Management of acne. CMAJ.https://pubmed.ncbi.nlm.nih.gov/21398228/
- Gollnick H, et al. (2003). Management of acne. JAAD.https://pubmed.ncbi.nlm.nih.gov/12734496/
- Thiboutot DM, et al. (2009). New insights into acne management. JAAD.https://pubmed.ncbi.nlm.nih.gov/19467365/
- American Academy of Dermatology. Pimple popping: Why only a dermatologist should do it.https://www.aad.org/public/diseases/acne/skin-care/popping
- Bowe WP, Shalita AR. (2008). Effective over-the-counter acne treatments. Seminars in Cutaneous Medicine and Surgery.https://pubmed.ncbi.nlm.nih.gov/18786497/
- Webster GF. (2005). The pathophysiology of acne. Cutis.https://pubmed.ncbi.nlm.nih.gov/15916220/
- Leyden JJ. (1995). New understandings of the pathogenesis of acne. JAAD.https://pubmed.ncbi.nlm.nih.gov/7775256/
Read This Next

Acne Face Mapping: Does Where You Break Out Tell You Why?

PCOS and Acne in Teens: When Breakouts Signal Something Bigger
If your acne won't respond to normal treatments and comes with irregular periods, it might be PCOS. Here's what teen girls and their parents need to know about diagnosis and treatment.
Read More →
Testosterone and Acne: Why Hormones Drive Most Teen Breakouts
Testosterone gets converted to DHT, which ramps up your oil glands. This is the core reason acne peaks during puberty and why boys tend to get it worse than girls.
Read More →
Inflammatory Acne: Papules, Pustules, and Why Your Skin Hurts
Inflammatory acne is the red, painful kind that actually hurts. Understanding the immune response behind it changes how you treat it and helps you stop making it worse.
Read More →
Comedonal Acne: Why Your Skin Is Bumpy But Not Red (And How to Fix It)
Comedonal acne gives you textured, bumpy skin without the redness of typical pimples. It's frustrating because it doesn't respond to the usual treatments. Here's what actually works.
Read More →