Whiteheads (Closed Comedones): What They Are, Why They Form, and How to Get Rid of Them
Medically reviewed by Dr. Sarah Mitchell, MD, Board-Certified Dermatologist
Written by Teen Acne Solutions Editorial Team — Updated March 17, 2026
Key takeaways
- Whiteheads are closed comedones — pores clogged with oil and dead skin cells sealed beneath the surface
- They look like small flesh-colored or white bumps, often clustered on the forehead, chin, and cheeks
- Squeezing whiteheads almost always makes them worse and can cause scarring
- Retinoids (like adapalene) are the gold standard treatment because they promote cell turnover
- Most whiteheads respond well to consistent treatment within 6-8 weeks
You run your fingers across your forehead and feel them — dozens of tiny, stubborn bumps that you can't quite see from a distance but are impossible to ignore up close. They're not red. They're not painful. They won't pop no matter how hard you try. And somehow, they seem to multiply overnight.
If this sounds familiar, you're dealing with whiteheads, also known as closed comedones — one of the most common and most misunderstood forms of acne, especially during the teen years. They're frustrating because they don't behave like "normal" pimples, and many of the standard acne-fighting tactics you've tried probably haven't worked on them.
The good news? Once you understand what's actually happening inside your skin, getting rid of whiteheads becomes much more straightforward. In this guide, we'll break down exactly what closed comedones are, why they form, and the step-by-step treatment approach that dermatologists recommend.

What Are Whiteheads
Let's start with the basics. A whitehead is a type of non-inflammatory acne lesion — technically called a closed comedone (plural: comedones). The word "comedone" comes from the Latin comedere, meaning "to eat up," which early physicians used to describe the way these lesions seemed to consume the skin.
Unlike the angry red pimples most people picture when they think of acne, whiteheads sit quietly beneath the surface. They're small, flesh-colored or slightly white bumps, usually 1-2 millimeters in diameter, with a smooth or slightly rounded top. You might barely see them in the mirror, but you can definitely feel them when you run your hand across your skin.
The Anatomy of a Closed Comedone
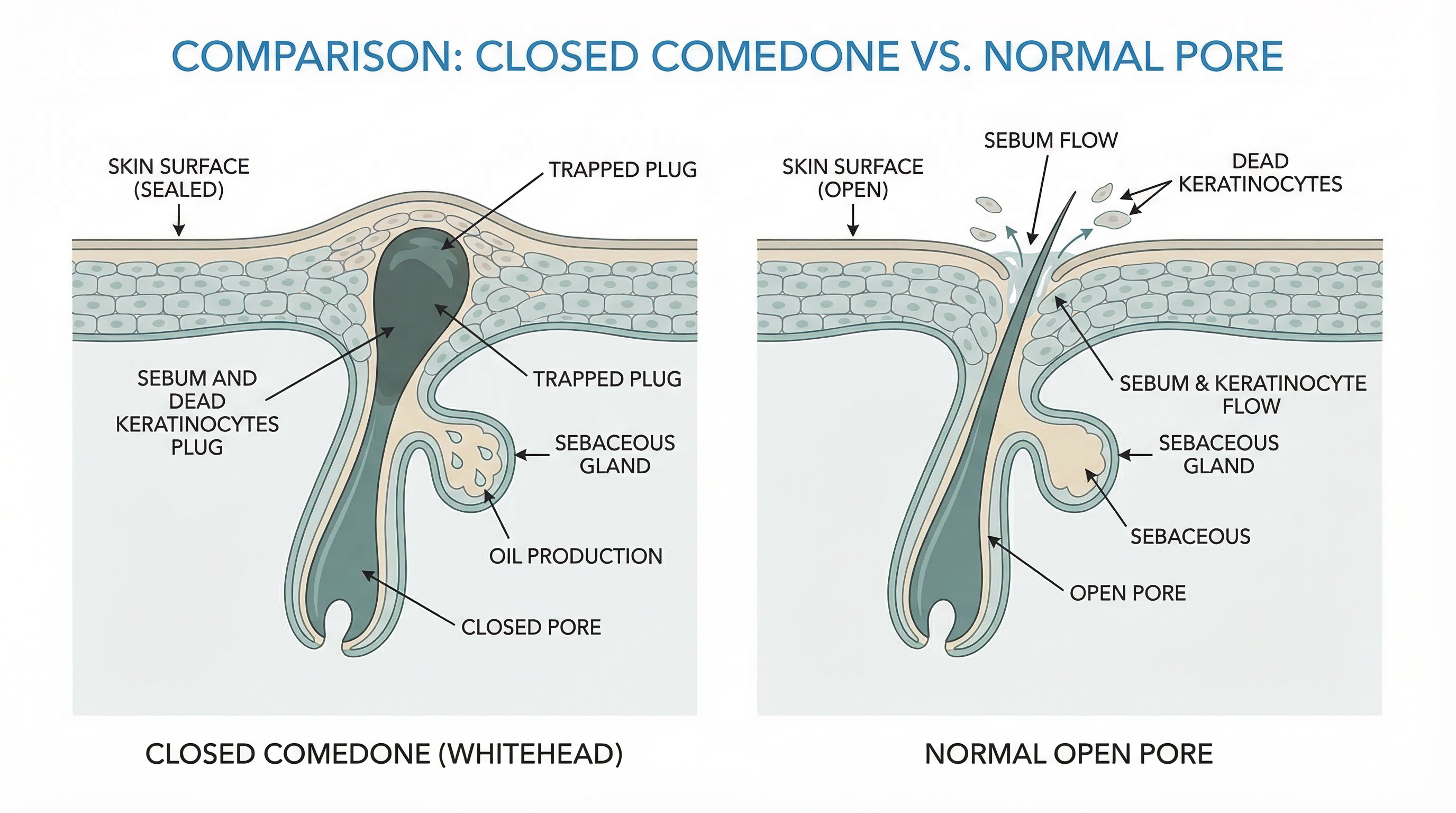
To understand whiteheads, you need to understand what's happening inside the pore — and it's more complex than most people realize.
Your skin is covered in tiny openings called pores (technically, pilosebaceous units). Each pore contains a hair follicle and a sebaceous gland, which produces an oily substance called sebum. Under normal circumstances, sebum travels up through the pore and onto the surface of your skin, where it helps keep your skin moisturized and protected.
Here's where things go wrong with closed comedones:
- The sebaceous gland overproduces sebum. This is especially common during puberty, when hormonal changes kick oil production into high gear.
- Dead skin cells don't shed properly. Instead of sloughing off the way they should, skin cells (called keratinocytes) inside the pore become sticky and clump together.
- A plug forms. The combination of excess sebum and sticky dead skin cells creates a dense keratin-and-sebum plug that blocks the pore opening.
- The pore stays sealed. Unlike a blackhead, where the pore remains open and the plug is exposed to air (causing it to oxidize and turn dark), a whitehead forms when a thin layer of skin grows over the top of the clogged pore, trapping everything underneath.
This is the critical distinction. A closed comedone is essentially a sealed pocket of oil, dead skin cells, and sometimes bacteria sitting just below the skin's surface. The contents have nowhere to go — they can't drain on their own, and the overlying skin keeps them locked in place.
Whiteheads vs. Other Types of Acne
Understanding how whiteheads differ from other acne lesions helps explain why they need a different treatment approach:
Whiteheads (Closed Comedones) vs. Blackheads (Open Comedones) Both are comedones — non-inflammatory clogged pores. The difference is simple: blackheads have an open pore, so the plug is exposed to oxygen and oxidizes, turning dark brown or black. Whiteheads have a closed pore, so the plug remains trapped under the surface and stays white or flesh-colored. Neither type is caused by dirt.
Whiteheads vs. Pustules ("Regular Pimples") Pustules are what most people mean when they say "pimple" — those red, swollen bumps with a visible white or yellow center of pus. Pustules are inflammatory, meaning bacteria (typically Cutibacterium acnes) have triggered an immune response. Whiteheads are non-inflammatory — there's no redness, swelling, or pus involved. However, whiteheads can progress into pustules if bacteria colonize the trapped plug and trigger inflammation.
Whiteheads vs. Milia This is a common source of confusion. Milia are tiny, hard, white bumps that look similar to whiteheads but are actually small cysts filled with trapped keratin (not sebum). Milia tend to appear around the eyes and cheeks, feel very firm, and don't respond to acne treatments. If your bumps are extremely hard and have been there for months without changing, they might be milia rather than whiteheads.
Whiteheads vs. Fungal Acne (Pityrosporum Folliculitis) Fungal acne presents as uniform, small, itchy bumps that can look a lot like closed comedones. The difference? Fungal acne is caused by an overgrowth of yeast, not clogged pores, and it itches — true whiteheads almost never itch. Fungal acne also doesn't respond to standard acne treatments and requires antifungal medication instead.
What Causes Whiteheads
Closed comedones don't appear randomly. They're the result of specific biological and environmental factors coming together. Here are the main culprits:
Hormonal Changes
This is the number one reason teens develop whiteheads. During puberty, your body ramps up production of androgens — hormones like testosterone and DHEA-S that directly stimulate your sebaceous glands to produce more oil. More oil means more raw material for pore-clogging plugs to form.
Hormonal fluctuations also affect how skin cells behave inside the pore. Research shows that androgens can increase the rate of follicular keratinization — the process by which skin cells inside the pore lining become sticky and accumulate instead of shedding normally. This double effect (more oil + stickier cells) is why acne peaks during the teen years.
For those who menstruate, monthly hormonal shifts can also trigger whiteheads. Many people notice new closed comedones appearing in the week before their period, when progesterone levels rise and stimulate oil production.
Excess Sebum Production
Even outside of hormonal fluctuations, some people simply produce more sebum than others. This is largely genetic. If your parents dealt with oily skin and acne during their teens, there's a good chance you will too. Sebum production can also increase in hot, humid weather, which is why many people notice more whiteheads during summer months.
Abnormal Desquamation (Dead Skin Cell Buildup)
Desquamation is the natural process of shedding dead skin cells. In people prone to comedones, this process goes haywire inside the hair follicle. Instead of shedding individually and exiting the pore, dead keratinocytes clump together in a process called retention hyperkeratosis. These clumps mix with sebum and form the characteristic comedonal plug.
This is a key concept for treatment: you can reduce oil all you want, but if the dead skin cell problem isn't addressed, whiteheads will keep forming.
Comedogenic Products
Not all skincare and cosmetic products are created equal. Some contain ingredients that are comedogenic — meaning they have a tendency to clog pores. Common comedogenic offenders include:
- Heavy mineral oil and petroleum-based products
- Coconut oil (despite its popularity in DIY skincare)
- Certain silicones (like dimethicone in heavy concentrations)
- Isopropyl myristate and isopropyl palmitate
- Cocoa butter and shea butter (in high concentrations)
- Some sunscreen formulations, especially thicker, cream-based ones
Hair products can also contribute, especially if you use heavy gels, pomades, or leave-in conditioners that transfer to your forehead and temples while you sleep. This is sometimes called pomade acne or acne cosmetica.
Other Contributing Factors
- Friction and pressure (from helmets, headbands, phone screens, or resting your chin on your hands) can worsen comedone formation in specific areas
- Diet may play a role — some research links high-glycemic diets and dairy consumption to increased acne, though the evidence is stronger for inflammatory acne than comedonal acne
- Stress can elevate cortisol levels, which may indirectly increase sebum production
- Certain medications, including some birth control pills, corticosteroids, and lithium, can promote comedone formation
How to Identify Whiteheads
What Whiteheads Look Like
Closed comedones have a distinctive appearance once you know what to look for:
- Size: Usually 1-3 millimeters in diameter — about the size of a pinhead
- Color: Flesh-colored, white, or very slightly yellowish
- Texture: Smooth, rounded bumps that feel firm (not soft or fluid-filled)
- Surface: Skin covers the top completely — there is no visible opening or "head"
- Inflammation: None — no redness, swelling, or tenderness
- Grouping: Often appear in clusters rather than as isolated bumps
They're sometimes most visible in certain lighting conditions. Try looking at your skin in natural sidelight (standing next to a window) or using a mirror with bright overhead light. The shadows cast by the bumps often make them more apparent.
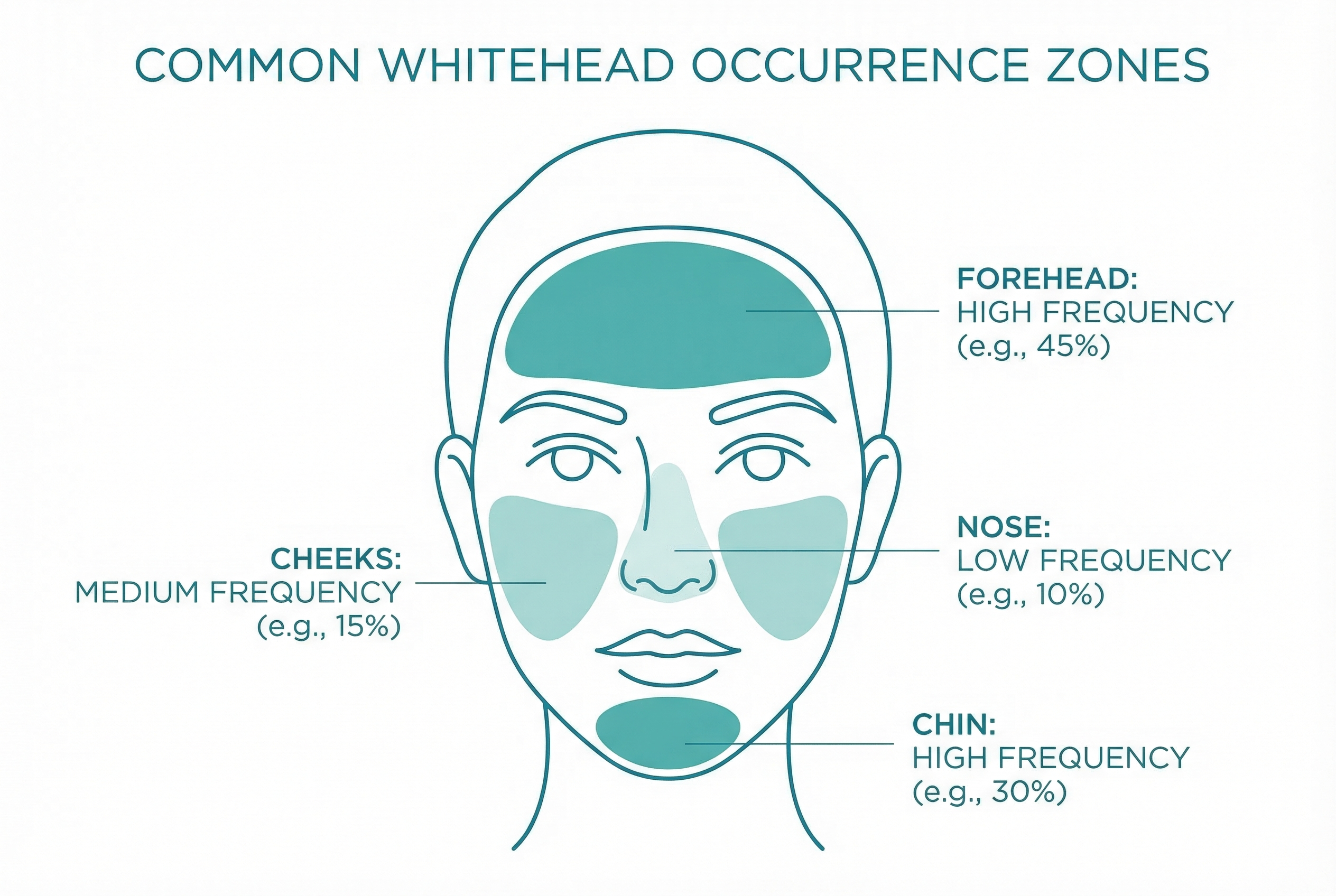
Common Locations
Whiteheads on the forehead are extremely common in teens, but closed comedones can appear anywhere you have oil-producing pores:
- Forehead: The most common location, especially along the hairline and between the eyebrows. The forehead belongs to the T-zone, which has a high concentration of sebaceous glands.
- Chin and jawline: Another T-zone hotspot, and an area particularly affected by hormonal fluctuations.
- Cheeks: Especially the inner cheeks near the nose. Cheek comedones can sometimes be related to comedogenic products or pillowcase hygiene.
- Nose: Though blackheads are more common here (because the pores on the nose tend to be larger and more open), whiteheads can form on and around the nose.
- Around the mouth: Sometimes related to lip balm, toothpaste, or other products that come into contact with this area.
Why You Shouldn't Squeeze Whiteheads
We know — it's tempting. The bumps are right there, and it feels like if you could just squeeze hard enough, the plug would come out and the bump would flatten. But squeezing whiteheads almost always backfires, and here's why:
The pore is sealed shut. Unlike a pustule that has a thin wall ready to rupture, a closed comedone is covered by intact skin. When you squeeze, the pressure has to go somewhere — and it usually goes deeper into the skin rather than outward. This can:
- Rupture the follicle wall below the surface, spilling the contents (oil, dead cells, bacteria) into the surrounding tissue
- Trigger an inflammatory response, transforming a calm, non-inflamed whitehead into an angry, red, swollen papule or even a cyst
- Introduce bacteria from your fingers into the damaged area, increasing the risk of infection
- Cause post-inflammatory hyperpigmentation (dark spots) or permanent scarring
In other words, squeezing a whitehead can turn a minor cosmetic concern into a much bigger skin problem. The dermatological consensus is clear: leave them alone and treat them with the right products instead.
Treatment Options
Treating closed comedones requires a different mindset than treating inflamed acne. The goal isn't to kill bacteria or reduce inflammation — it's to unclog the pore from the inside out by promoting normal skin cell turnover and reducing excess oil. Here's the treatment ladder that dermatologists recommend, starting with the most accessible options.
Step 1: Salicylic Acid (Over-the-Counter)
Salicylic acid is often the best starting point for mild whiteheads. It's a beta-hydroxy acid (BHA) that works in two important ways:
- It's oil-soluble, meaning it can penetrate into the pore and dissolve the mix of sebum and dead skin cells that make up the comedonal plug
- It has mild anti-inflammatory properties that help keep things calm
Look for a leave-on product (cleanser, toner, or serum) with 0.5-2% salicylic acid. Leave-on formulations are more effective than wash-off cleansers because the active ingredient stays in contact with your skin longer.
How to use it: Apply once daily to start (at night), then increase to twice daily if your skin tolerates it. You may notice some mild dryness or peeling in the first week or two — this is normal and usually subsides.
Timeline: Give salicylic acid at least 4-6 weeks of consistent use before evaluating results. Comedones are slow to respond.
Step 2: Retinoids (The Gold Standard)
If salicylic acid alone isn't enough — or if you have moderate to widespread closed comedones — retinoids are the next step and are considered the gold standard treatment for comedonal acne by virtually every major dermatology guideline.
Retinoids work by:
- Normalizing follicular keratinization — they "reprogram" the skin cells lining the pore to shed properly instead of clumping together
- Accelerating cell turnover — old, dead cells are replaced more quickly, preventing plug formation
- Reducing microcomedone formation — they address the earliest, invisible stage of comedone development, preventing new whiteheads before they even become visible
Over-the-counter option: Adapalene 0.1% (Differin) Adapalene became available without a prescription in the United States in 2016, and it's a game-changer for treating whiteheads. It's a third-generation retinoid that's effective yet better tolerated than older retinoids like tretinoin.
How to use adapalene:
- Cleanse your face with a gentle, non-comedogenic cleanser
- Wait until your skin is completely dry (10-15 minutes) — applying to damp skin increases irritation
- Apply a pea-sized amount to your entire face (not just the areas with whiteheads) — retinoids work by preventing new comedones everywhere
- Follow with a non-comedogenic moisturizer
- Use only at night — retinoids can increase sun sensitivity
- Wear broad-spectrum sunscreen (SPF 30+) every morning
The retinoid "purge": During the first 2-4 weeks, you may notice your skin looks worse before it looks better. This is sometimes called the "retinoid purge" — existing microcomedones (tiny, invisible pre-comedones already forming in your pores) are being pushed to the surface faster. This is actually a sign the medication is working. Stick with it.
Prescription options: If OTC adapalene isn't strong enough, a dermatologist can prescribe stronger concentrations (adapalene 0.3%) or other retinoids like tretinoin (Retin-A) or tazarotene (Tazorac). These are more potent but also more irritating, so they require careful introduction and monitoring.
Step 3: Combination Therapy
For stubborn whiteheads that resist single-agent treatment, dermatologists often recommend combining active ingredients:
- Adapalene + benzoyl peroxide: Available as a combination product (Epiduo), this pairs the comedone-fighting power of a retinoid with benzoyl peroxide's ability to kill acne bacteria and reduce the risk of comedones progressing to inflammatory lesions.
- Retinoid + salicylic acid: Using a salicylic acid product in the morning and a retinoid at night can provide dual comedone-clearing action. However, introduce them one at a time to avoid overwhelming your skin.
- Azelaic acid: Available in OTC (10%) and prescription (15-20%) strengths, azelaic acid normalizes keratinization and has anti-inflammatory properties. It's a good option for people who can't tolerate retinoids.
Professional Extraction
A board-certified dermatologist or trained esthetician can perform professional comedone extraction — a procedure where whiteheads are carefully opened with a sterile instrument (often a small needle or lancet) and the contents are gently expressed using a comedone extractor tool.
This is fundamentally different from squeezing at home because:
- The skin is properly prepared (often with a chemical peel or steam first)
- Sterile instruments are used to create a precise, controlled opening
- Proper technique minimizes tissue damage and scarring risk
- It's done in a clean environment, reducing infection risk
Professional extraction provides immediate results but is not a long-term solution on its own — without ongoing topical treatment to prevent new comedones from forming, they'll come right back.
Chemical Peels
In-office chemical peels using glycolic acid, salicylic acid, or other agents can help treat widespread closed comedones by removing the top layer of skin and unclogging pores en masse. These are typically done in a series of sessions spaced 2-4 weeks apart and work well as a complement to daily topical treatment.

Prevention Strategies
Treating existing whiteheads is only half the battle. Preventing new ones from forming is equally important — and much easier once you build the right habits.
Build a Non-Comedogenic Skincare Routine
The single most impactful prevention strategy is ensuring that every product that touches your face is non-comedogenic (meaning it's been formulated not to clog pores). This includes:
- Cleanser: Use a gentle, fragrance-free, non-comedogenic cleanser twice daily. Avoid harsh scrubs and "squeaky clean" cleansers that strip your skin — they can trigger rebound oil production that makes things worse.
- Moisturizer: Yes, even oily, acne-prone skin needs moisturizer. Look for lightweight, oil-free, non-comedogenic formulas. Gel-based moisturizers are often a good choice for oily skin.
- Sunscreen: Choose oil-free, non-comedogenic sunscreen with SPF 30 or higher. Mineral (zinc oxide/titanium dioxide) formulations are often better tolerated by acne-prone skin than chemical sunscreens.
- Makeup: If you wear makeup, choose non-comedogenic, oil-free formulas. Always remove makeup thoroughly before bed — sleeping in makeup is a recipe for comedone formation.
Practice Gentle Exfoliation
Regular, gentle exfoliation helps prevent the dead skin cell buildup that leads to comedones. A BHA (salicylic acid) product used 2-3 times per week can help keep pores clear even after your existing whiteheads have resolved. Some people benefit from alternating with an AHA (glycolic or lactic acid) product for surface-level exfoliation.
Avoid physical scrubs with large, rough particles — they can create micro-tears in the skin and actually worsen acne. If you want a physical exfoliant, look for gentle options with fine, round particles.
Manage Oil Production
While you can't fundamentally change how much sebum your skin produces (that's largely genetic and hormonal), you can manage excess oil:
- Blotting papers absorb surface oil without disturbing your skincare or makeup
- Oil-free products across your entire routine help reduce the total oil burden on your skin
- Niacinamide (vitamin B3) in concentrations of 2-5% has been shown to help regulate sebum production and is well-tolerated by most skin types
- Resist the urge to over-wash — washing your face more than twice daily strips natural oils and triggers your skin to compensate by producing even more
Watch Your Hair Products
If your whiteheads are concentrated on your forehead, temples, or along the hairline, your hair products might be the culprit. Shampoos, conditioners, styling products, and hair oils can transfer to your skin, especially overnight. Try:
- Washing your face after rinsing out conditioner in the shower
- Keeping heavy styling products away from your hairline
- Changing your pillowcase at least once a week (or placing a clean t-shirt over your pillow)
- Pulling your hair back off your face when you sleep
Don't Touch Your Face
Your hands carry oils, bacteria, and dirt that can transfer to your facial skin and contribute to pore clogging. Be mindful of habits like resting your chin on your hands, pressing your phone against your cheek, or picking at your skin. If you find yourself touching your face frequently, keeping your hands busy with a small object (like a stress ball) can help break the habit.
Common Myths About Whiteheads
Myth: Whiteheads are caused by poor hygiene. Fact: Whiteheads form because of internal factors — excess oil production, abnormal skin cell behavior, and hormonal influences. You cannot wash them away, and over-cleansing actually makes them worse. A person with impeccable hygiene can still develop closed comedones.
Myth: You need to "dry out" your skin to get rid of whiteheads. Fact: Aggressively drying out your skin with alcohol-based products or harsh treatments damages your skin barrier and triggers compensatory oil production. Well-hydrated skin with a healthy barrier actually produces less excess oil than dehydrated skin.
Myth: Whiteheads are just "baby acne" and you'll grow out of them. Fact: While many teens do see their acne improve as they move through puberty and hormones stabilize, closed comedones can persist well into adulthood if not properly treated. Waiting it out without treatment also increases the risk that whiteheads will progress into inflammatory acne.
Myth: Toothpaste is an effective spot treatment for whiteheads. Fact: Toothpaste contains ingredients like sodium lauryl sulfate, menthol, and fluoride that can irritate the skin and actually worsen acne. It has no comedolytic (pore-unclogging) properties. Stick with proven active ingredients like salicylic acid and retinoids.
Myth: Sun exposure clears up whiteheads. Fact: While a tan may temporarily mask the appearance of whiteheads, UV exposure actually thickens the outer layer of skin (stratum corneum), which can worsen pore clogging and lead to a breakout weeks later. UV damage also increases the risk of post-inflammatory hyperpigmentation. Always wear sunscreen.
Myth: If a product doesn't work in a week, it's not going to work. Fact: Comedonal acne is notoriously slow to respond to treatment. Skin cells take approximately 28 days to complete their turnover cycle, and it typically takes 6-8 weeks of consistent use before you see significant improvement with most acne treatments. Patience and consistency are essential.
When to See a Dermatologist
While many cases of mild whiteheads respond well to over-the-counter treatments, there are situations where professional help is the smart move:
- OTC treatments haven't worked after 8-12 weeks of consistent use
- Whiteheads are widespread — covering most of your forehead, cheeks, or chin
- Comedones keep progressing into inflamed pimples, painful nodules, or cysts
- You're developing scarring or persistent dark marks from your acne
- Your acne is significantly affecting your self-esteem or mental health — this is a completely valid reason to seek help, and don't let anyone tell you otherwise
- You suspect your bumps might not be whiteheads — conditions like milia, fungal acne, keratosis pilaris, and flat warts can mimic closed comedones and require different treatments
- You're considering prescription-strength retinoids or other treatments that require medical supervision
A dermatologist can confirm your diagnosis, rule out lookalike conditions, and create a personalized treatment plan that may include prescription retinoids, hormonal treatments (for those who menstruate), or in-office procedures like extractions and chemical peels.
What to Expect at Your Appointment
If you've never seen a dermatologist before, here's what a typical first visit for acne looks like:
- Medical history: The doctor will ask about your acne history, current skincare routine, any products you've tried, medications you're taking, and family history of acne.
- Skin examination: They'll examine your skin closely, often using magnification, to assess the type, severity, and distribution of your acne.
- Treatment plan: Based on their assessment, they'll recommend a treatment approach, which typically includes a combination of topical medications and skincare adjustments.
- Follow-up: Most dermatologists want to see you back in 6-8 weeks to assess how your skin is responding and make any necessary adjustments.
Come prepared with a list of every product you currently use on your face (or take photos of the product labels), as well as any questions you have. The more information you provide, the better your dermatologist can tailor their recommendations.
The Bottom Line
Whiteheads might not be as dramatic-looking as inflamed pimples, but they can be just as frustrating — especially when they cover your forehead or cheeks in a stubborn, textured layer that won't budge. The key to clearing them is understanding that closed comedones are a pore-clogging problem, not an infection or inflammation problem, and treating them accordingly.
Start with a gentle, non-comedogenic skincare routine and a salicylic acid product. If that's not enough after 4-6 weeks, step up to a retinoid like over-the-counter adapalene. Be patient, be consistent, and resist the urge to squeeze. Most people see meaningful improvement within 6-8 weeks of starting the right treatment — and with ongoing prevention habits, those small bumps can become a thing of the past.
Your skin is worth the patience. And if you're struggling or unsure, a dermatologist can help you find the right path forward — there's no reason to fight this battle alone.
This article is for informational purposes only and does not constitute medical advice. Always consult a board-certified dermatologist or healthcare provider for personalized acne treatment recommendations.
How we reviewed this article:
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
- Zaenglein AL, et al. (2016). Guidelines of care for the management of acne vulgaris. Journal of the American Academy of Dermatology.https://pubmed.ncbi.nlm.nih.gov/26897386/
- Thiboutot DM, et al. (2009). New insights into the management of acne. Journal of the American Academy of Dermatology.https://pubmed.ncbi.nlm.nih.gov/19467365/
- Leyden JJ. (1995). New understandings of the pathogenesis of acne. Journal of the American Academy of Dermatology.https://pubmed.ncbi.nlm.nih.gov/7775256/
- Dréno B, et al. (2015). Understanding innate immunity and inflammation in acne. Journal of the European Academy of Dermatology.https://pubmed.ncbi.nlm.nih.gov/25382740/
- Gollnick H, et al. (2003). Management of acne: A report from the Global Alliance. Journal of the American Academy of Dermatology.https://pubmed.ncbi.nlm.nih.gov/12734496/
- American Academy of Dermatology. Acne: Overview.https://www.aad.org/public/diseases/acne
- Cunliffe WJ, Holland DB, Jeremy A. (2004). Comedone formation: Etiology, clinical presentation, and treatment. Clinics in Dermatology.https://pubmed.ncbi.nlm.nih.gov/15556729/
- Del Rosso JQ. (2009). The role of skin care as an integral component in the management of acne vulgaris. Journal of Clinical and Aesthetic Dermatology.https://pubmed.ncbi.nlm.nih.gov/20729948/
- Kraft J, Freiman A. (2011). Management of acne. Canadian Medical Association Journal.https://pubmed.ncbi.nlm.nih.gov/21398228/
- Webster GF. (2005). The pathophysiology of acne. Cutis.https://pubmed.ncbi.nlm.nih.gov/15916220/
Read This Next

Acne Face Mapping: Does Where You Break Out Tell You Why?

PCOS and Acne in Teens: When Breakouts Signal Something Bigger
If your acne won't respond to normal treatments and comes with irregular periods, it might be PCOS. Here's what teen girls and their parents need to know about diagnosis and treatment.
Read More →
Testosterone and Acne: Why Hormones Drive Most Teen Breakouts
Testosterone gets converted to DHT, which ramps up your oil glands. This is the core reason acne peaks during puberty and why boys tend to get it worse than girls.
Read More →
Inflammatory Acne: Papules, Pustules, and Why Your Skin Hurts
Inflammatory acne is the red, painful kind that actually hurts. Understanding the immune response behind it changes how you treat it and helps you stop making it worse.
Read More →
Comedonal Acne: Why Your Skin Is Bumpy But Not Red (And How to Fix It)
Comedonal acne gives you textured, bumpy skin without the redness of typical pimples. It's frustrating because it doesn't respond to the usual treatments. Here's what actually works.
Read More →