Papules: Understanding Small Red Acne Bumps and How to Treat Them
Medically reviewed by Dr. Sarah Mitchell, MD, Board-Certified Dermatologist
Written by Teen Acne Solutions Editorial Team — Updated March 15, 2026
Key takeaways
- Papules are small (under 5mm), red, inflamed bumps WITHOUT a visible white or yellow head
- They form when a clogged pore's wall breaks down, triggering your immune system's inflammatory response
- Never try to pop a papule — there's nothing to extract, and squeezing drives bacteria deeper
- Benzoyl peroxide and topical retinoids are the most effective treatments for papular acne
- Papules signal the transition from mild (comedonal) to moderate (inflammatory) acne
You look in the mirror and notice a cluster of small, red, tender bumps on your cheek. They're not whiteheads — there's no visible head to speak of. They're not deep, throbbing cysts either. They just sit there, flushed and angry, and when you press on one it hurts more than you expected.
Those bumps are called papules, and they represent one of the most important turning points in acne. When papules show up, your skin is telling you that what started as simple clogged pores has crossed a line into something more serious: inflammatory acne.
If you're a teen dealing with these frustrating red bumps, you're far from alone. Papular acne is one of the most common forms of inflammatory acne during adolescence, and understanding exactly what's happening inside your skin is the first step toward getting it under control. In this guide, we'll break down what papules are, why they form, how they differ from other types of acne, and — most importantly — the treatments that actually work.
What Are Papules?
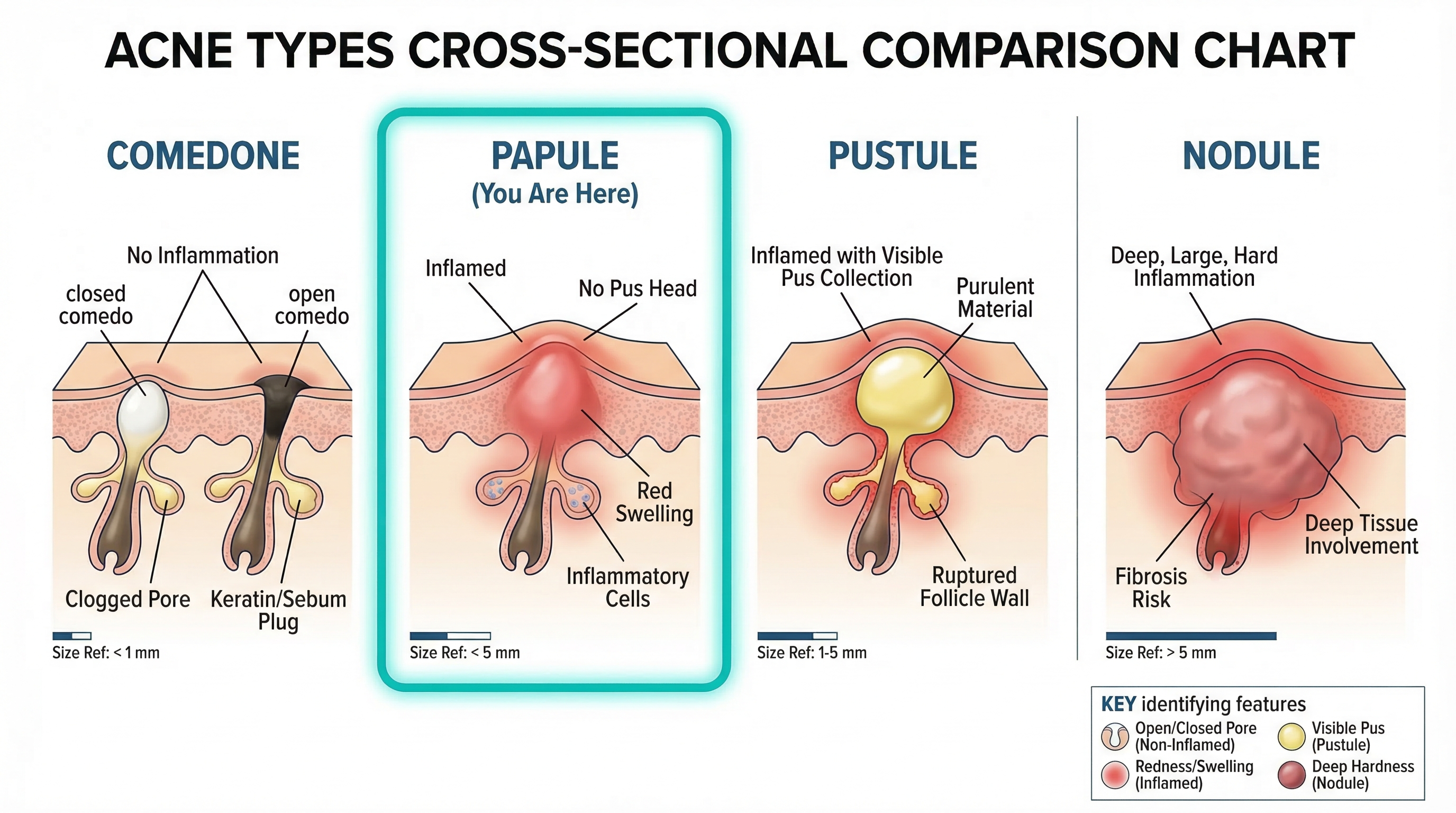
A papule is a small, solid, raised bump on the skin that is typically less than 5 millimeters in diameter — roughly the size of a pencil eraser or smaller. In the context of acne, papules are inflamed lesions that appear red or pink on lighter skin tones and may appear darker or purplish-brown on deeper skin tones. They feel firm to the touch, and they're usually tender or mildly painful when pressed.
The defining characteristic that separates papules from many other acne types is what they don't have: a visible white or yellow head. Unlike pustules (which contain a visible pocket of pus at the surface) or whiteheads (which have a thin layer of skin covering a plug of sebum and dead cells), papules are solid bumps with all of the inflammation happening beneath the surface.
Here's a quick clinical snapshot of what makes a papule a papule:
- Size: Under 5mm in diameter
- Color: Red, pink, or darkened depending on skin tone
- Texture: Firm and raised, with no soft or fluid-filled center
- Head: None visible — no white tip, no yellow pus
- Sensation: Tender to the touch, sometimes mildly painful
- Location: Commonly appears on the face (especially the forehead, cheeks, and chin), but can develop on the back, chest, and shoulders
When dermatologists evaluate acne severity, the presence of papules is a key indicator. Papules signal that your acne has moved beyond the comedonal stage (blackheads and whiteheads only) into the inflammatory stage — and that distinction matters for treatment.
How Papules Form: The Inflammatory Cascade
To understand papules, you need to understand what happens when a simple clogged pore goes wrong. The journey from a quiet comedone to an angry red papule is a multi-step process, and it involves your immune system in a way that blackheads and whiteheads do not.
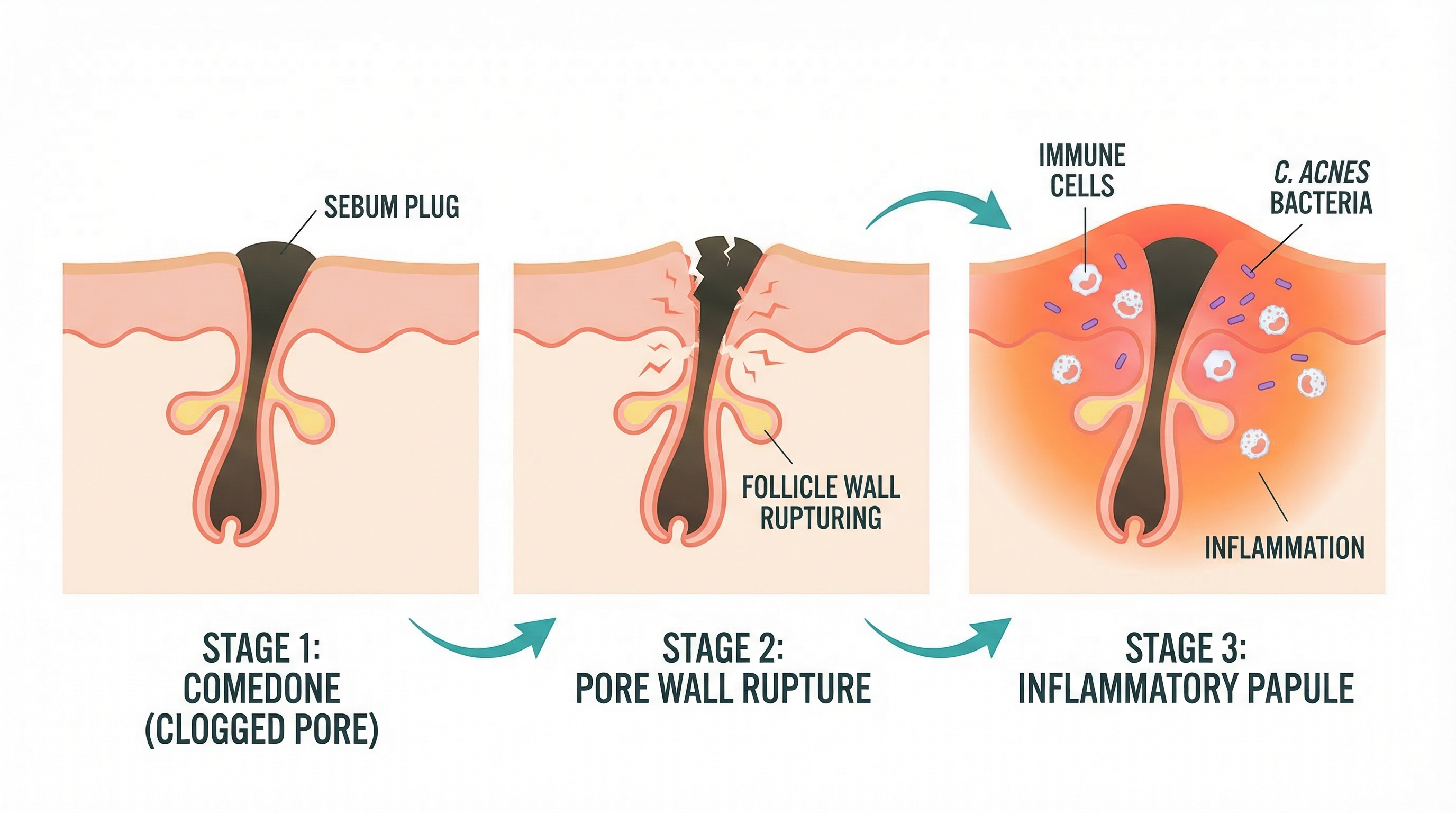
Step 1: The Clogged Pore
Every papule starts its life as a microcomedone — a pore that has become clogged with a mixture of excess sebum (oil), dead skin cells, and debris. During puberty, surging androgen hormones stimulate your sebaceous glands to produce more oil than your pores can handle. At the same time, the skin cells lining the inside of the follicle become stickier than usual and don't shed properly. The result is a plug that blocks the pore opening.
At this stage, you might see a blackhead (open comedone) or a whitehead (closed comedone) — or the clog might be so small it's invisible to the naked eye.
Step 2: Bacterial Overgrowth
Trapped behind that plug, conditions inside the pore become ideal for Cutibacterium acnes (C. acnes), the bacterium that lives naturally on everyone's skin. In an open, well-ventilated pore, C. acnes populations stay in check. But in a sealed, oil-rich environment, these bacteria multiply rapidly.
As C. acnes feeds on the trapped sebum, it produces inflammatory byproducts — including enzymes called lipases that break down triglycerides into free fatty acids, which are highly irritating to surrounding tissue. The bacteria also release proteins that act as chemical signals, essentially waving a red flag to your immune system.
Step 3: The Pore Wall Breaks Down
Here's where the transition from comedone to papule actually happens. As pressure builds inside the clogged pore — from accumulated oil, dead cells, and bacterial colonies — the wall of the follicle weakens and eventually ruptures. This doesn't happen at the skin's surface (that would be more like a popped pimple). Instead, the rupture happens deep within the dermis, spilling the contents of the pore — bacteria, sebum, dead cells, and all those inflammatory byproducts — into the surrounding tissue.
This is the critical moment. What was once contained inside a single pore is now loose in the surrounding skin.
Step 4: The Immune Response
Your body treats that ruptured pore contents like an invasion. The immune system launches an inflammatory response, flooding the area with white blood cells (primarily neutrophils and macrophages) to contain and destroy the foreign material. Blood vessels in the area dilate to allow more immune cells to arrive, which is why the area turns red and feels warm.
This inflammatory cascade is what produces the visible papule: a firm, red, swollen bump that represents your immune system actively fighting the infection beneath the surface. The tenderness you feel is the result of inflammatory mediators — chemicals like cytokines and prostaglandins — sensitizing the nerve endings in the area.
Importantly, at the papule stage, the immune response hasn't yet produced a significant collection of pus. The white blood cells are still arriving and working. If enough pus accumulates and pushes toward the surface, the papule may eventually evolve into a pustule (that classic "pimple with a head"). But many papules resolve on their own without ever forming a visible head — the immune system clears the debris internally.
Papules vs. Other Acne Types: How to Tell Them Apart
One of the most common questions we hear is: "How do I know if I have papules or something else?" Acne comes in several forms, and knowing which type you're dealing with helps you choose the right treatment. Here's how papules compare to every other major acne lesion.
Papules vs. Whiteheads (Closed Comedones)
Whiteheads are non-inflammatory clogged pores covered by a thin layer of skin. They appear as small, flesh-colored or slightly white bumps. They don't hurt, they're not red, and they don't involve an immune response. Papules, by contrast, are red, tender, and swollen. If a whitehead's follicle wall ruptures and triggers inflammation, that whitehead has effectively become a papule.
Papules vs. Blackheads (Open Comedones)
Blackheads are open clogged pores where the plug is exposed to air, causing oxidation that turns it dark. Like whiteheads, they're non-inflammatory. They don't hurt and aren't red. Papules are the inflammatory step that can follow if a blackhead's pore wall breaks down beneath the surface.
Papules vs. Pustules
This is the comparison that trips people up the most. Both papules and pustules are inflammatory acne lesions, and they're often found side by side on the same face. The key difference is the visible head: pustules have a distinct white or yellowish tip where pus has collected near the surface. Papules do not. Think of pustules as the next stage — when a papule's immune response produces enough pus to become visible. Not all papules progress to pustules, however. Many resolve without ever developing a head.
Papules vs. Nodules
Nodules are larger (over 5mm), deeper, and more painful than papules. While a papule sits relatively close to the surface and feels like a firm bump, a nodule is a hard, painful lump that extends deep into the dermis or even the subcutaneous tissue. Nodules represent a more severe inflammatory response and are much more likely to cause scarring. If your red bumps are large, deeply embedded, and extremely painful, they may be nodules rather than papules — and that distinction calls for different (often prescription-only) treatment.
Papules vs. Cysts
Cystic acne produces large, soft, fluid-filled or semi-solid lumps beneath the skin. Cysts are typically the most severe form of acne, and they feel different from papules — where papules are firm and relatively small, cysts feel more like a soft, swollen mass under the skin. Cysts almost always require professional dermatological treatment and carry a high risk of scarring.
Quick Comparison Chart
| Feature | Papule | Pustule | Whitehead | Blackhead | Nodule | Cyst |
|---|---|---|---|---|---|---|
| Size | < 5mm | < 5mm | 1-3mm | 1-3mm | > 5mm | > 5mm |
| Color | Red/pink | Red with white tip | Flesh/white | Dark | Red/skin-colored | Red/skin-colored |
| Head visible? | No | Yes (white/yellow) | No | Yes (dark) | No | No |
| Painful? | Mildly | Mildly | No | No | Very | Very |
| Inflammatory? | Yes | Yes | No | No | Yes | Yes |
| Depth | Shallow-mid | Shallow | Surface | Surface | Deep | Deep |
Where Papules Fit on the Acne Grading Scale
Dermatologists use acne grading systems to assess severity and determine appropriate treatment. While several classification systems exist, most follow a similar pattern:
- Grade I (Mild/Comedonal): Mostly blackheads and whiteheads with very few inflammatory lesions. The skin may look bumpy but isn't particularly red or painful.
- Grade II (Moderate/Papular): This is where papules enter the picture. A noticeable number of papules and pustules are present alongside comedones. The acne is visibly red and inflamed in patches.
- Grade III (Moderately Severe/Pustular): Widespread papules and pustules, potentially with a few nodules. Multiple areas of the face or body are affected.
- Grade IV (Severe/Nodulocystic): Numerous nodules and cysts in addition to papules and pustules. High risk of scarring.
If your acne is predominantly papular — clusters of small red pimples with no head, scattered across your cheeks, forehead, or jawline — you're likely in the Grade II range. This is clinically significant because Grade II is typically where dermatologists begin recommending active treatment beyond basic face washing. It's the point where a good skincare routine alone may not be enough, and targeted anti-acne ingredients become important.
Why You Should Never Pop a Papule
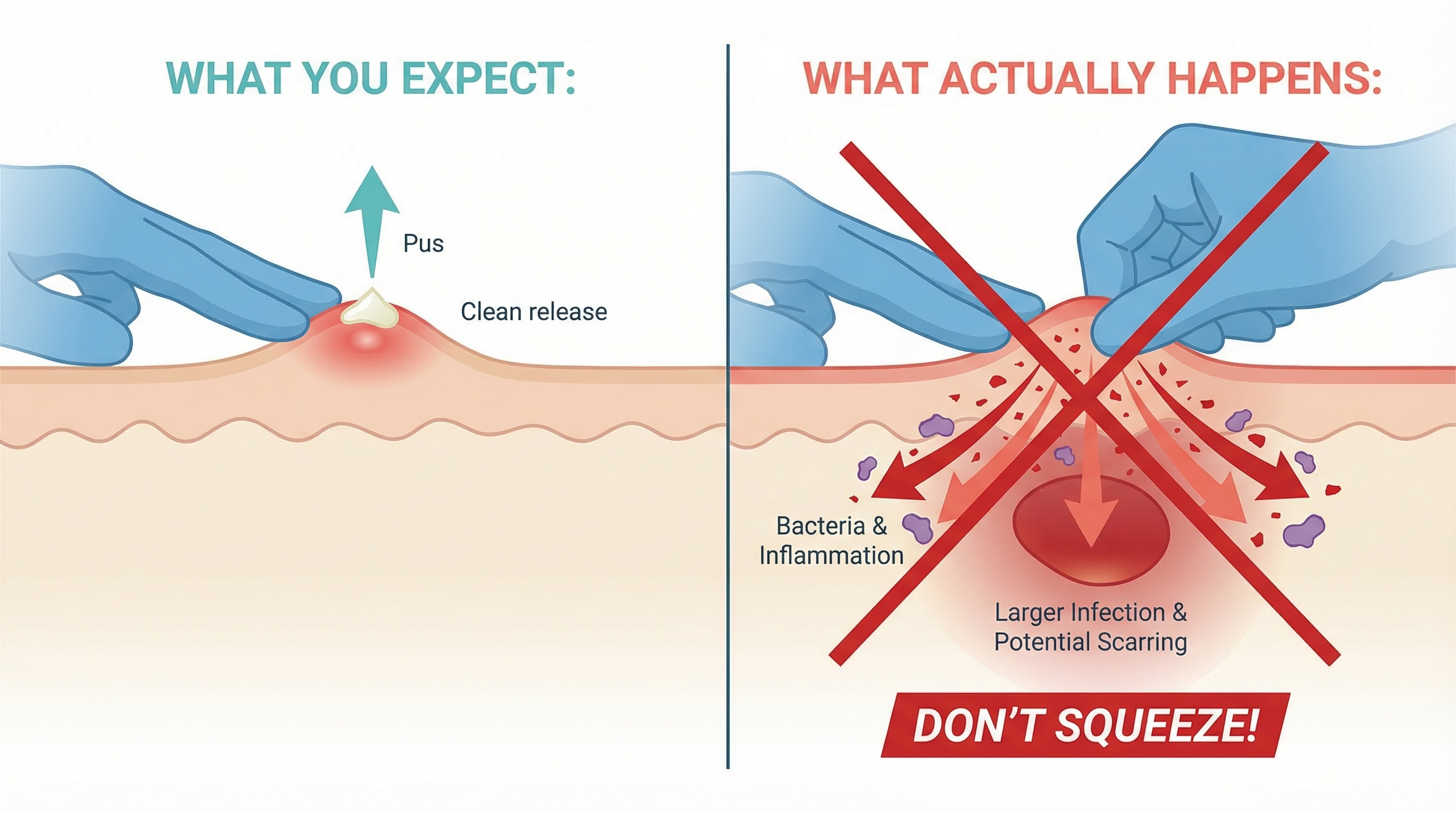
We get it. When you see a red bump on your face, the instinct to squeeze it is almost overwhelming. But with papules, popping isn't just inadvisable — it's physically pointless and actively harmful.
There's Nothing to Pop
A pustule has a visible pocket of pus near the surface that (in theory) can be expressed. A papule does not. When you squeeze a papule, there's no pus to come out. What you're actually doing is compressing inflamed tissue against itself, which increases pressure in an area that's already under stress.
You're Pushing Bacteria Deeper
When you apply pressure to a papule, you risk rupturing the follicle wall further — not toward the surface, but deeper into the dermis. This drives bacteria, inflammatory debris, and immune cells into surrounding tissue, effectively spreading the infection sideways and downward. The result is often a larger and more painful lesion than what you started with, and in some cases, a single squeezed papule can trigger multiple new breakouts in the surrounding area.
You're Increasing Scarring Risk
Every time you traumatize inflamed skin through picking or squeezing, you increase the likelihood of post-inflammatory hyperpigmentation (PIH) — those dark marks that linger long after the acne itself has healed — and atrophic scarring (permanent pitting or indentation). For teens with deeper skin tones, PIH from manipulated papules can persist for months or even years.
What to Do Instead
If a papule is bothering you, here are safer alternatives:
- Apply a cold compress or ice cube wrapped in a thin cloth for 1-2 minutes. This constricts blood vessels and can temporarily reduce redness and swelling.
- Apply a spot treatment with benzoyl peroxide (2.5-5%) directly to the papule.
- Use a hydrocolloid patch — while these are designed for pus-filled lesions, they can protect papules from picking and create a moist healing environment.
- Leave it alone. Most papules resolve within 5-7 days with proper skincare.
Treatment Options for Papular Acne
Treating papules effectively means addressing the underlying drivers of inflammatory acne: excess oil production, bacterial overgrowth, abnormal skin cell turnover, and inflammation itself. Here are the most effective treatment approaches, organized from over-the-counter options to prescription therapies.
Over-the-Counter Treatments
Benzoyl Peroxide (2.5%-10%)
Benzoyl peroxide is widely considered the single most effective OTC ingredient for inflammatory acne, including papules. It works through multiple mechanisms: it kills C. acnes bacteria on contact through oxidation, it helps reduce inflammation, and — unlike topical antibiotics — bacteria cannot develop resistance to it.
For papular acne, most dermatologists recommend starting with a 2.5% or 5% concentration. Research has consistently shown that 2.5% benzoyl peroxide is nearly as effective as 10% with significantly less irritation — an important consideration for teen skin, which is often sensitive and reactive.
How to use it: Apply a thin layer to affected areas (not just individual papules) once daily, preferably in the evening. Start with every other day if your skin is sensitive, and build up to daily use over two weeks. Benzoyl peroxide can bleach fabrics, so use white pillowcases and towels.
Salicylic Acid (0.5%-2%)
Salicylic acid is a beta-hydroxy acid (BHA) that works by dissolving the bonds between dead skin cells inside the pore, helping to unclog blockages. It also has mild anti-inflammatory properties. While salicylic acid is generally more effective for comedonal acne (blackheads and whiteheads), it plays a supporting role in papular acne by helping prevent the clogged pores that eventually become papules.
How to use it: Available in cleansers, toners, and leave-on treatments. A 2% salicylic acid cleanser used once daily is a good starting point. It can be combined with benzoyl peroxide, but introduce products one at a time to monitor for irritation.
Adapalene 0.1% (Differin)
Adapalene is a topical retinoid that is now available over the counter, and it's a genuine game-changer for papular acne. Retinoids work by normalizing skin cell turnover inside the follicle, preventing the clogged pores that lead to papules in the first place. Adapalene also has direct anti-inflammatory effects, making it particularly well-suited for inflammatory papular acne.
How to use it: Apply a pea-sized amount to the entire face (not just spots) once daily in the evening, after cleansing and before moisturizer. Expect a retinization period of 2-6 weeks where your skin may get temporarily worse (more dryness, peeling, and possibly more breakouts) before it gets better. This is normal and expected. Full results typically take 8-12 weeks.
Important: Adapalene increases sun sensitivity. Daily sunscreen (SPF 30+) is non-negotiable while using this product.
Prescription Treatments
If OTC options aren't delivering sufficient improvement after 8-12 weeks of consistent use, it's time to see a dermatologist. Prescription options for papular acne include:
Prescription-Strength Retinoids
Tretinoin (Retin-A) and tazarotene are stronger retinoids available by prescription. They work on the same principles as adapalene but may be more effective for stubborn papular acne. Your dermatologist will determine the appropriate strength and formulation based on your skin type and acne severity.
Topical Antibiotics
Clindamycin and erythromycin are topical antibiotics that reduce C. acnes populations and have anti-inflammatory effects. However, they should almost never be used alone due to the risk of bacterial resistance. Dermatologists typically prescribe them in combination with benzoyl peroxide — in fact, several combination products (like clindamycin/benzoyl peroxide gel) are available as a single formulation for convenience.
Combination Therapy
For moderate papular acne, the most effective approach is usually a combination regimen. A common evidence-based protocol looks like this:
- Morning: Gentle cleanser, then benzoyl peroxide (or a benzoyl peroxide/antibiotic combination), then moisturizer with SPF
- Evening: Gentle cleanser, then a topical retinoid (adapalene or tretinoin), then moisturizer
This two-pronged approach tackles acne from multiple angles — killing bacteria and reducing inflammation during the day, while normalizing cell turnover and preventing new comedones at night.
Oral Antibiotics
For widespread papular acne that isn't responding to topical treatments alone, dermatologists may prescribe a course of oral antibiotics such as doxycycline or minocycline. These are typically used for a limited period (3-6 months) to get inflammation under control, and they should always be used alongside topical treatments (especially benzoyl peroxide) to prevent resistance.
Hormonal Therapy
For teen girls and young women whose papular acne is driven primarily by hormonal fluctuations, oral contraceptives or spironolactone may be effective options. These work by reducing the androgen-driven sebum overproduction that starts the acne cascade. This is a conversation to have with both a dermatologist and a primary care provider.
Immediate Relief: Cold Compresses and Anti-Inflammatory Care
While your long-term treatment works, there are things you can do right now to calm inflamed papules:
- Ice or cold compress: Wrap an ice cube in a thin, clean cloth and hold it against the papule for 60-90 seconds. Wait a few minutes and repeat. Cold constricts blood vessels, reducing redness and swelling temporarily. Do not apply ice directly to skin.
- Niacinamide serum (2-5%): Niacinamide is an anti-inflammatory ingredient that helps calm redness and strengthen the skin barrier. It's well-tolerated by most skin types and can be layered under other treatments.
- Green tea extract: Some studies suggest that topical green tea (epigallocatechin gallate) has anti-inflammatory and antimicrobial properties that may help calm inflamed papules.
- Avoid hot water on your face. Lukewarm water is less likely to exacerbate inflammation and strip your skin barrier.
When Papules Signal You Need Stronger Treatment
Papules aren't just a type of acne — they're an indicator of where you stand on the acne severity spectrum. Their presence tells you and your dermatologist important things about what's happening in your skin and what treatment approach is warranted.
Red Flags to Watch For
Consider seeing a dermatologist if you notice any of the following:
- Papules that don't respond to 8-12 weeks of consistent OTC treatment. If you've been using benzoyl peroxide and/or adapalene daily for three months without meaningful improvement, you need a stronger approach.
- Papules that are progressing to nodules. If your red bumps are getting larger, deeper, and more painful over time, your acne may be advancing in severity.
- Widespread papules across multiple areas. A few papules on the chin are different from dense clusters across the cheeks, forehead, jawline, and back. Distribution and density both matter.
- Papules that leave marks. If every papule leaves a dark spot (post-inflammatory hyperpigmentation) or a small scar, proactive treatment is essential to prevent long-term skin damage.
- Papules accompanied by significant psychological distress. Acne's emotional impact is real and valid. If your skin is affecting your confidence, mood, or daily life, that alone is reason enough to seek professional help — regardless of how "severe" the acne looks objectively.
The Escalation Ladder
Dermatologists typically think about acne treatment as a ladder:
- Step 1: OTC benzoyl peroxide + adapalene (for mild-to-moderate papular acne)
- Step 2: Prescription retinoid + topical antibiotic/BPO combination (for moderate papular acne not responding to OTC)
- Step 3: Add oral antibiotics to the topical regimen (for moderately severe papular-pustular acne)
- Step 4: Consider isotretinoin (Accutane) or hormonal therapy (for severe or treatment-resistant acne)
The goal is always to use the least aggressive treatment that effectively controls your acne. But the key word is "effectively." Under-treating inflammatory acne like papules increases your risk of scarring, and scarring is much harder to address after the fact than the acne itself.
Preventing Papules: Building a Foundation
While you can't always prevent papules entirely — especially during the hormonal upheaval of adolescence — you can create conditions that make them less likely to form and easier to manage when they do.
Skincare Basics That Actually Matter
- Cleanse twice daily with a gentle, non-comedogenic cleanser. Harsh scrubs and strong cleansers strip the skin barrier, which paradoxically triggers more oil production and more inflammation. Look for terms like "gentle," "non-foaming" or "low-foam," and "pH-balanced."
- Moisturize every day, even if your skin is oily. A lightweight, oil-free moisturizer helps maintain the skin barrier, reducing the irritation and inflammation that contribute to papule formation. Skipping moisturizer because your skin is oily is one of the most common — and most counterproductive — mistakes in teen skincare.
- Wear SPF 30+ sunscreen daily. Sun exposure increases inflammation and worsens post-inflammatory hyperpigmentation from healed papules. This is doubly important if you're using retinoids or benzoyl peroxide, both of which can increase sun sensitivity.
- Don't over-wash or over-exfoliate. Washing your face more than twice daily or using multiple exfoliating products simultaneously damages the skin barrier and can make papular acne worse, not better.
Lifestyle Factors
- Change pillowcases frequently — at least once or twice per week. Pillowcases accumulate oil, dead skin cells, and bacteria that can contribute to pore clogging.
- Keep your hands away from your face. Easier said than done, but habitual face-touching transfers bacteria and causes friction that can irritate existing papules and trigger new ones.
- Manage stress when possible. Stress hormones (particularly cortisol) can increase sebum production and inflammation, potentially worsening papular acne. This is especially relevant during exam periods and other high-stress times that are common in teen life.
- Be patient with treatment. The biggest reason acne treatments "fail" is that people abandon them too early. Most effective acne treatments take 6-12 weeks to show meaningful results. Switching products every week or two prevents anything from working.

The Bottom Line
Papules are more than just small red pimples with no head. They're your skin's signal that acne has crossed the threshold from simple clogged pores into active inflammatory disease. The redness, the tenderness, the firm little bumps that refuse to come to a head — all of that is your immune system responding to a pore wall that has broken down beneath the surface.
The good news is that papular acne is highly treatable. The combination of benzoyl peroxide and a topical retinoid like adapalene — both available without a prescription — is effective for most cases of mild-to-moderate papular acne. For more stubborn cases, dermatologists have an entire arsenal of prescription options that can bring inflammatory acne under control.
The most important thing you can do right now is resist the urge to pop, pick, or squeeze those papules. There's nothing inside them to extract, and manipulating them only drives bacteria deeper and increases your risk of lasting marks and scars. Instead, start a consistent treatment routine, give it the time it needs to work, and see a dermatologist if things aren't improving after two to three months.
Your skin is going through a lot right now — and so are you. Papular acne doesn't define you, it doesn't mean you're doing something wrong, and it absolutely can get better. The fact that you're here, learning about what's happening in your skin and what you can do about it, is already the right first step.
How we reviewed this article:
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
- Zaenglein AL, et al. (2016). Guidelines of care for the management of acne vulgaris. JAAD.https://pubmed.ncbi.nlm.nih.gov/26897386/
- Dréno B, et al. (2015). Understanding innate immunity and inflammation in acne. JEADV.https://pubmed.ncbi.nlm.nih.gov/25382740/
- Gollnick H, et al. (2003). Management of acne. JAAD.https://pubmed.ncbi.nlm.nih.gov/12734496/
- Leyden JJ. (1995). New understandings of the pathogenesis of acne. JAAD.https://pubmed.ncbi.nlm.nih.gov/7775256/
- Kraft J, Freiman A. (2011). Management of acne. CMAJ.https://pubmed.ncbi.nlm.nih.gov/21398228/
- Thiboutot DM, et al. (2009). New insights into acne management. JAAD.https://pubmed.ncbi.nlm.nih.gov/19467365/
- Webster GF. (2005). The pathophysiology of acne. Cutis.https://pubmed.ncbi.nlm.nih.gov/15916220/
- American Academy of Dermatology. Acne: Overview.https://www.aad.org/public/diseases/acne
- Del Rosso JQ. (2009). The role of skin care in acne management. JCAD.https://pubmed.ncbi.nlm.nih.gov/20729948/
- Tanghetti EA. (2013). The role of inflammation in the pathology of acne. Journal of Clinical and Aesthetic Dermatology.https://pubmed.ncbi.nlm.nih.gov/24062871/
Read This Next

Acne Face Mapping: Does Where You Break Out Tell You Why?

PCOS and Acne in Teens: When Breakouts Signal Something Bigger
If your acne won't respond to normal treatments and comes with irregular periods, it might be PCOS. Here's what teen girls and their parents need to know about diagnosis and treatment.
Read More →
Testosterone and Acne: Why Hormones Drive Most Teen Breakouts
Testosterone gets converted to DHT, which ramps up your oil glands. This is the core reason acne peaks during puberty and why boys tend to get it worse than girls.
Read More →
Inflammatory Acne: Papules, Pustules, and Why Your Skin Hurts
Inflammatory acne is the red, painful kind that actually hurts. Understanding the immune response behind it changes how you treat it and helps you stop making it worse.
Read More →
Comedonal Acne: Why Your Skin Is Bumpy But Not Red (And How to Fix It)
Comedonal acne gives you textured, bumpy skin without the redness of typical pimples. It's frustrating because it doesn't respond to the usual treatments. Here's what actually works.
Read More →