Hormonal Acne Patterns: How to Identify Hormone-Driven Breakouts by Location and Timing
Medically reviewed by Dr. Rachel Torres, MD, Pediatric Dermatologist
Written by Teen Acne Solutions Editorial Team — Updated March 10, 2026
Key takeaways
- Hormonal acne typically concentrates on the lower face — jawline, chin, and lower cheeks
- In girls, cyclical breakouts that appear 7-10 days before menstruation are a hallmark of hormonal acne
- In boys, hormonal acne is often more widespread and severe due to higher androgen levels
- Face mapping has some scientific basis — different facial zones do have different hormonal sensitivity
- If your acne follows a predictable pattern by location or timing, hormonal factors are likely involved
If you have ever noticed that your breakouts always seem to cluster in the same spots — along your jawline, on your chin, or deep on your lower cheeks — you are not imagining things. The location, timing, and character of your acne can tell you a surprising amount about what is driving it beneath the surface. And for many teenagers, the answer comes down to one word: hormones.
This guide is not about treatment (we cover that in depth in our hormonal acne treatment guide). Instead, this is about learning to read your skin — understanding the visual patterns and timing clues that distinguish hormonal acne from other types, so you can have a more informed conversation with your dermatologist and take control of your skincare approach.
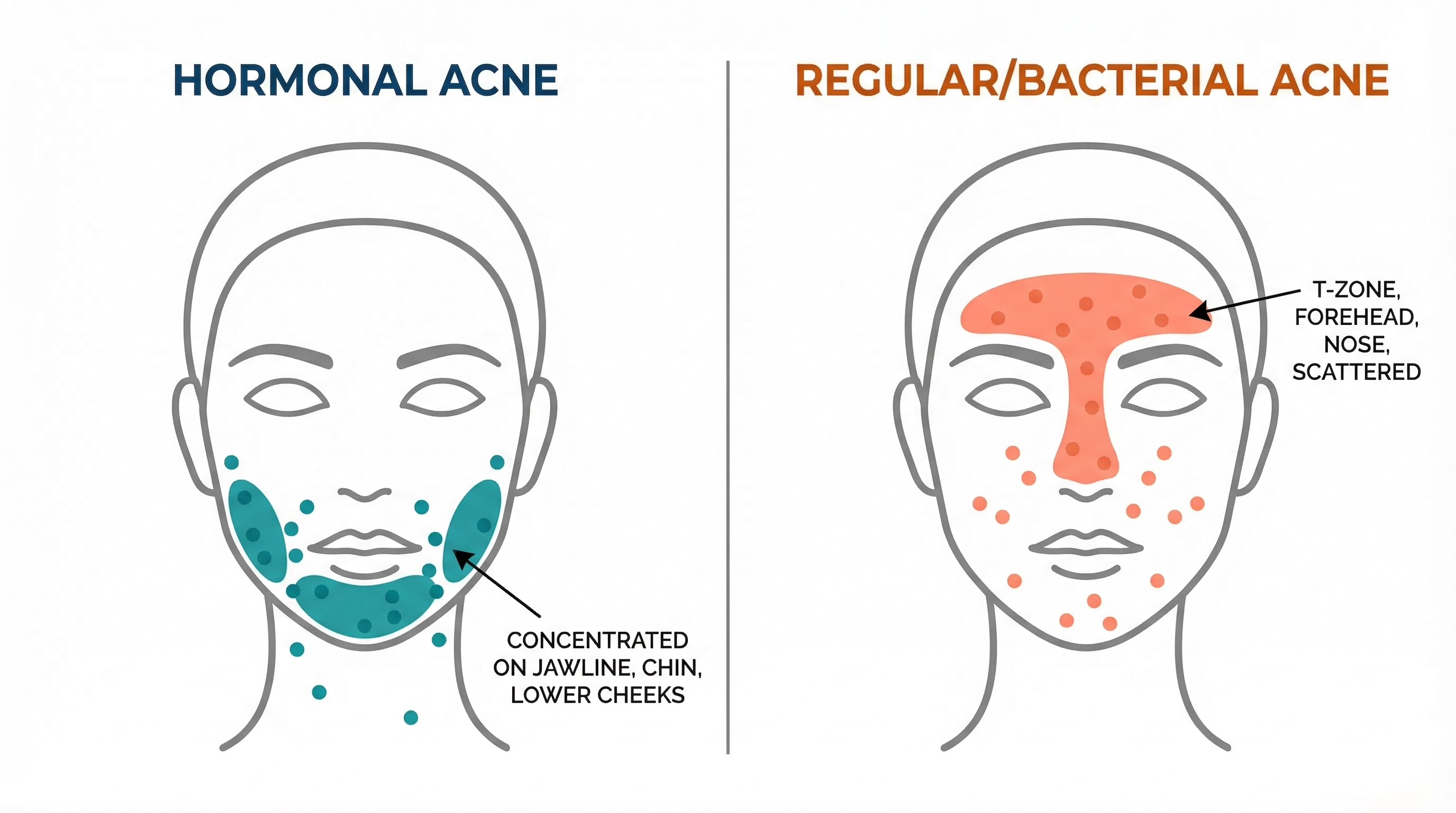
 Common zones where hormonal acne concentrates. The lower third of the face — jawline, chin, and lower cheeks — is the classic hormonal territory.
Common zones where hormonal acne concentrates. The lower third of the face — jawline, chin, and lower cheeks — is the classic hormonal territory.
What Makes Acne "Hormonal"
Technically, almost all acne has a hormonal component. Your sebaceous (oil-producing) glands require hormonal signaling to function at all. But when dermatologists use the term "hormonal acne," they are referring to breakouts that are primarily driven by fluctuations or elevated levels of specific hormones — particularly androgens.
The Hormones Behind the Breakouts
Three androgens play the biggest roles in acne development during the teen years:
DHEA-S (dehydroepiandrosterone sulfate) is often the first androgen to rise during puberty, sometimes years before other visible signs of development appear. Produced by the adrenal glands, DHEA-S is frequently the hormone responsible for the very earliest acne breakouts — sometimes appearing in children as young as 8 or 9. Research by Lucky et al. (1994) found that rising DHEA-S levels correlated with the onset of comedonal acne even before menarche in girls.
Testosterone increases significantly during puberty in both sexes, though boys produce roughly 10 times more than girls. It stimulates sebaceous glands to enlarge and produce more sebum. In girls, even small fluctuations in testosterone — particularly the "free" unbound form — can trigger noticeable breakouts.
DHT (dihydrotestosterone) is the most potent androgen affecting the skin. The enzyme 5-alpha reductase converts testosterone into DHT directly within the skin's sebaceous glands. DHT is estimated to be 5 to 10 times more potent than testosterone at stimulating oil production. Critically, research by Thiboutot (2004) demonstrated that androgen receptor density and 5-alpha reductase activity vary across different facial zones — a finding that helps explain why hormonal acne favors certain locations.
Why Location Matters
Here is the key insight: your sebaceous glands are not distributed evenly across your face, and neither are the androgen receptors that control them. The lower face — particularly the jawline and chin — has a higher density of androgen receptors compared to the forehead or mid-cheeks. This means that when androgen levels rise or fluctuate, the lower face responds more dramatically with increased oil production, clogged pores, and inflammatory breakouts.
This biological reality is what gives hormonal acne its characteristic pattern. It is not random — it is a map of your skin's hormonal sensitivity.
The Jawline and Chin Pattern
The single most recognizable pattern of hormonal acne is breakouts concentrated along the jawline, chin, and lower cheeks. If you drew a U-shape from one ear, down along the jaw, across the chin, and back up to the other ear, you would be tracing the classic hormonal acne zone.
What Jawline Acne Looks Like
Hormonal acne in this zone tends to have specific characteristics that set it apart from other types:
- Deep, cystic lesions. Rather than surface-level whiteheads or blackheads, hormonal jawline acne often presents as painful, deep nodules or cysts beneath the skin. These take longer to develop, last longer, and are more likely to leave marks.
- Fewer but larger bumps. You might not have dozens of pimples — instead, you may get 3 to 5 significant, stubborn lesions that linger for weeks.
- Tenderness before visibility. Hormonal cysts often announce themselves with deep tenderness or a dull ache before any visible bump appears on the surface.
- Resistance to topical treatments. Because these lesions form deep in the dermis, standard over-the-counter treatments that work on surface acne often have limited effect.
Why the Jawline Specifically
The jawline and chin area has the highest concentration of androgen receptors on the face. When circulating androgen levels rise — as they do cyclically before menstruation, during puberty surges, or due to conditions like PCOS — these receptors activate the sebaceous glands in that zone more aggressively than elsewhere. The result is localized overproduction of sebum, which mixes with dead skin cells to clog pores, creating an environment where Cutibacterium acnes bacteria thrive and trigger inflammation.
Research published in Clinics in Dermatology (Ju et al., 2017) confirmed that the distribution of sex hormone receptors in the skin is not uniform, and that this non-uniformity directly corresponds to common acne distribution patterns.
Cyclical Breakouts in Girls
For many teenage girls and young women, the most telling sign of hormonal acne is not just where it appears, but when it appears. If your breakouts arrive on a roughly monthly schedule, you are almost certainly dealing with hormone-driven acne.
The Premenstrual Flare Pattern
Research by Geller et al. (2014) found that up to 65% of women and girls with acne report premenstrual worsening of their breakouts. The pattern typically looks like this:
- Days 1-14 of the cycle (follicular phase): Skin is relatively clear. Estrogen levels are rising, which has a mildly protective effect against acne.
- Days 14-21 (ovulation and early luteal phase): Progesterone rises, which can cause mild water retention and early pore swelling. Some people notice a slight increase in oiliness.
- Days 21-28 (late luteal phase, roughly 7-10 days before menstruation): This is when hormonal breakouts characteristically appear. Estrogen drops while progesterone and androgens remain relatively elevated. The ratio shift favors androgen activity, and the lower face responds.
- Days 1-5 (menstruation): Breakouts may peak during the first few days of the period, then gradually begin to resolve.
How to Confirm the Cyclical Pattern
The best way to determine whether your acne is cyclically hormonal is to track it. For at least two to three full cycles, note:
- When new breakouts appear (exact dates)
- Where they appear (which zones of the face)
- What type they are (surface pimple, deep cyst, cluster of small bumps)
- Where you are in your menstrual cycle
After two to three months, a clear pattern usually emerges. Many teens find it helpful to use a period-tracking app that also allows symptom logging, or simply to keep a brief daily skin journal.
 A typical cyclical breakout pattern. Notice how breakouts concentrate in the late luteal phase, approximately 7-10 days before the period begins.
A typical cyclical breakout pattern. Notice how breakouts concentrate in the late luteal phase, approximately 7-10 days before the period begins.
Hormonal Acne in Boys vs. Girls
Hormonal acne affects both sexes during the teen years, but it presents quite differently due to the dramatically different hormonal profiles of male and female puberty.
Boys: More Widespread, Often More Severe
Teenage boys produce significantly higher levels of testosterone and DHT than girls, and their acne patterns reflect this:
- Distribution is more diffuse. Rather than concentrating on the lower face, boys' hormonal acne tends to spread across the entire face — forehead, cheeks, nose, chin, and jawline. It also more frequently involves the back (often called "bacne"), chest, and shoulders.
- Onset is often more sudden and intense. Boys frequently experience a rapid escalation in acne severity that correlates with the pubertal testosterone surge, typically between ages 12 and 16.
- The pattern is less cyclical. Without a monthly hormonal cycle, boys' hormonal acne tends to be more persistent and less predictable in its timing. It may worsen gradually and then plateau rather than waxing and waning monthly.
- Severity tends to be greater. Epidemiological data from Bhate and Williams (2013) shows that severe acne (nodulocystic) is more common in males, which correlates with their higher androgen levels.
Girls: More Localized, More Predictable
In contrast, girls' hormonal acne tends to be:
- Concentrated on the lower face. The jawline-chin pattern described above is significantly more common in female hormonal acne.
- Cyclical and somewhat predictable. The menstrual cycle creates a repeating pattern that, once identified, can be anticipated.
- Characterized by fewer but deeper lesions. Girls are more likely to develop isolated deep cysts rather than widespread moderate acne.
- Persistent beyond the teen years. Research by Preneau and Dreno (2012) found that female acne often persists or even begins in the late teens and twenties, while male acne more commonly peaks in mid-adolescence and then improves.
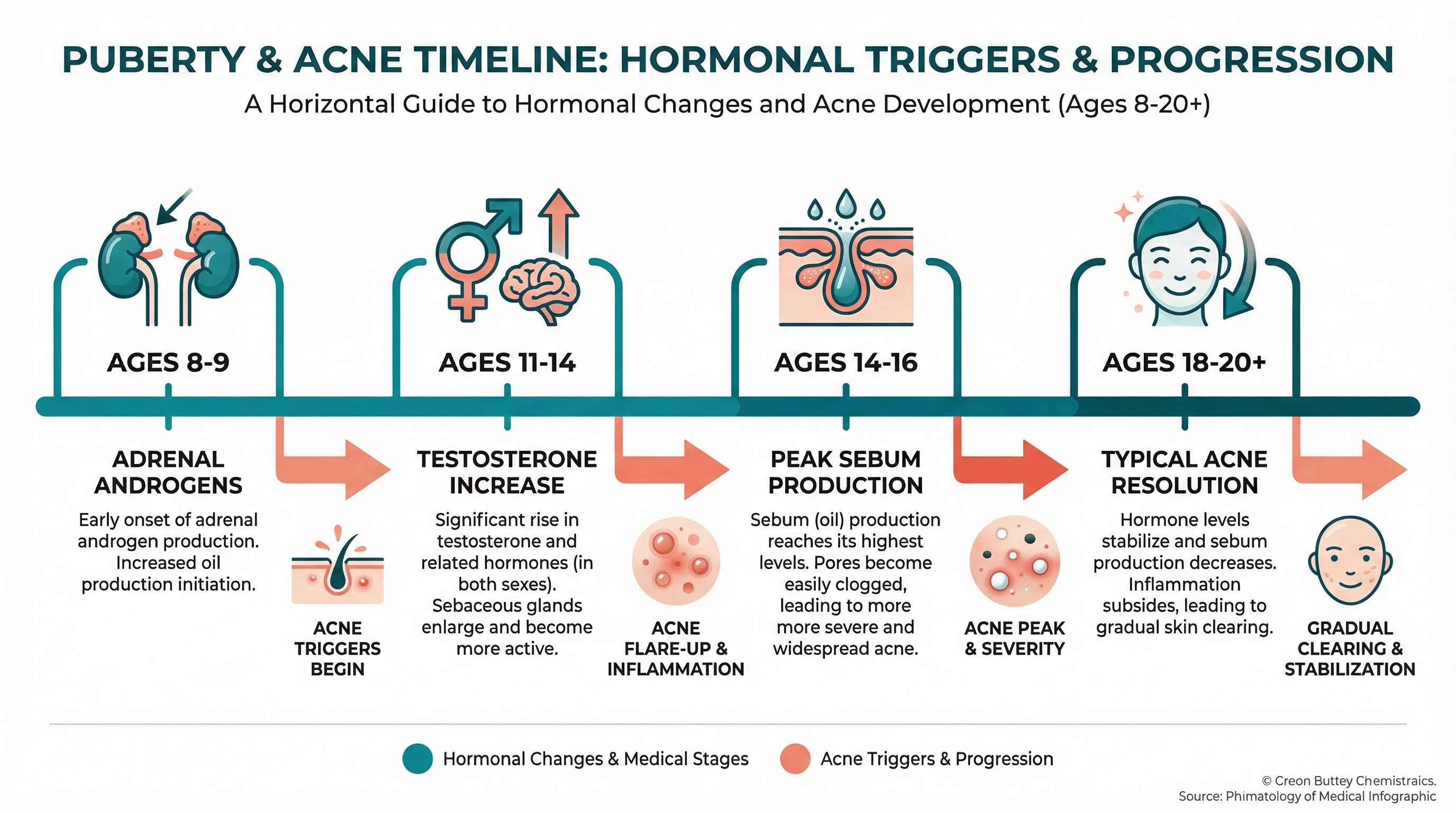
The Puberty Timeline
Understanding when hormonal acne typically appears can help you identify it:
- Girls, ages 8-11: The earliest acne (usually comedonal — blackheads and whiteheads on the forehead and nose) often appears as DHEA-S rises during adrenarche, sometimes years before the first period.
- Girls, ages 11-14: As estrogen and testosterone both increase, acne may worsen and begin migrating toward the lower face.
- Boys, ages 11-14: Acne onset, often starting with comedones on the forehead and nose, progressing to inflammatory lesions across the face.
- Boys, ages 14-17: Peak acne severity for many boys, corresponding to the testosterone surge. Back and chest involvement becomes more common.
Face Mapping: What's Real and What's Myth
You have probably seen face mapping charts on social media — diagrams dividing the face into zones and claiming each zone corresponds to an internal organ or specific health issue. The forehead supposedly reflects your digestive system, the cheeks your lungs, and so on. How much of this is actually true?
The Traditional Claims
Face mapping has roots in Traditional Chinese Medicine (TCM) and Ayurvedic medicine, where different facial zones supposedly correspond to internal organs: the forehead to the digestive system, the cheeks to the lungs, the nose to the heart, and the chin to the reproductive organs.
What Science Actually Supports
Modern dermatology does not support the idea that acne on your forehead means your liver is struggling or that cheek acne indicates a lung problem.
However, science does support a more nuanced version of zone-based acne interpretation:
- The lower face (jawline, chin) genuinely has higher androgen receptor density, making it legitimately more responsive to hormonal fluctuations. So the idea that chin acne relates to reproductive hormones has a real scientific basis — just not for the reasons traditional face mapping claims.
- The forehead and nose (T-zone) have the highest density of sebaceous glands, which is why these areas tend to be oiliest and why acne often starts here during early puberty when oil production first increases.
- Different facial zones have different exposure profiles. Cheek acne, for instance, can genuinely be influenced by phone contact, pillowcase hygiene, or mask-wearing — external factors that affect specific zones.
The Bottom Line on Face Mapping
Think of it this way: face mapping based on organ connections is largely myth. But face mapping based on androgen receptor distribution, sebaceous gland density, and external contact patterns is scientifically supported. Your breakout location does carry information — just not the mystical kind.
 Traditional face mapping vs. what dermatology actually supports. The lower face hormonal connection has real scientific backing, but claims about organ connections do not.
Traditional face mapping vs. what dermatology actually supports. The lower face hormonal connection has real scientific backing, but claims about organ connections do not.
Breakout Location Decoder
Use this guide to interpret what your breakout location may be telling you. Remember: these are tendencies, not rules. Individual variation exists, and many people have acne driven by multiple factors across different zones.
Jawline and Chin
Most likely driver: Hormonal (androgen-mediated)
Supporting clues: Deep, cystic lesions; cyclical pattern in girls; concentration along the U-zone of the lower face; resistance to standard topical treatments.
Other possibilities to rule out: Friction from chin straps, helmets, or musical instruments; resting your chin on your hands.
Cheeks
Most likely driver: A mix of hormonal and external factors
Supporting clues: Hormonal cheek acne tends to affect the lower cheeks and is often deeper and more inflammatory. External-factor cheek acne (phone, pillowcase, touching) tends to be more one-sided or clustered in specific spots.
Questions to ask yourself: Is it worse on the side you sleep on? The side you hold your phone to? Did it start when you began wearing a mask regularly?
Forehead
Most likely driver: Excess oil production, hair products, or cosmetics (comedogenic products)
Supporting clues: Forehead acne is common in early puberty when the T-zone oil production first ramps up. It is also frequently associated with hair products (pomade acne), bangs that trap oil and sweat against the skin, or heavy foundations.
Hormonal component: The forehead has high sebaceous gland density, so rising androgens during puberty do contribute — but pure hormonal acne in older teens that appears only on the forehead is less common.
Back and Chest
Most likely driver: Hormonal (especially in boys), friction, or sweat
Supporting clues: Back and chest acne correlates strongly with elevated androgens and is more common in males. It also worsens with heat, sweat, and tight clothing. If you get both face and body acne, hormonal factors are very likely involved.
Temples
Most likely driver: Hair products, headwear, or sweat
Supporting clues: Temple acne is frequently linked to hair oils, gels, or sprays that migrate onto the skin. Headbands, hats, and helmet straps can also cause acne mechanica in this zone.
Other Hormonal Acne Patterns
Beyond location, several other patterns can signal that hormones are a primary driver of your breakouts.
Stress-Triggered Flares
When you are stressed, your adrenal glands produce more cortisol and DHEA-S. Both can stimulate sebaceous glands and trigger breakouts. If your acne consistently worsens during exam periods, family stress, or emotional upheaval — and particularly if these stress breakouts favor the lower face — hormonal mechanisms are at play.
The stress-acne connection is not just "in your head." It is a measurable hormonal cascade: stress increases cortisol, which increases adrenal androgen output, which increases sebum production. The timeline is typically a 1-2 week delay between the stressful event and the resulting breakout.
Acne That Worsens with Certain Foods
While diet does not directly cause hormonal acne, certain foods can amplify hormonal signaling. High-glycemic foods cause insulin spikes, and insulin increases the bioavailability of androgens by reducing sex hormone-binding globulin (SHBG). Dairy — particularly skim milk — has also been associated with acne, potentially due to naturally present hormones.
Acne That Started Very Early
If your acne appeared before age 10, particularly if it was among the first signs of puberty, adrenal androgens (specifically DHEA-S) are almost certainly the driver. This pattern, sometimes called prepubertal acne, warrants evaluation by a pediatric dermatologist or endocrinologist to ensure it represents normal adrenarche rather than a hormonal abnormality.
When to Suspect PCOS or Other Hormonal Disorders
For most teenagers, hormonal acne is a normal — if frustrating — part of puberty. However, certain patterns should prompt a conversation with your doctor about possible underlying hormonal conditions.
Polycystic Ovary Syndrome (PCOS)
PCOS affects an estimated 6-12% of females of reproductive age and is a common cause of persistent hormonal acne. Suspect PCOS if you have acne combined with:
- Irregular or absent periods
- Excessive hair growth on the face, chest, or back (hirsutism)
- Hair thinning on the scalp
- Difficulty maintaining a healthy weight
- Acne that is unusually severe or completely unresponsive to standard treatments
Other Conditions to Consider
- Congenital adrenal hyperplasia (CAH): A genetic condition causing excess adrenal androgen production, presenting similarly to PCOS.
- Androgen-secreting tumors: Extremely rare, but sudden severe acne combined with rapid virilization (voice deepening, muscle changes) warrants urgent evaluation.
- Thyroid disorders and Cushing's syndrome: Both can affect skin health and acne patterns.
When to Get Hormone Testing
Not everyone with hormonal acne needs blood work. But hormone testing becomes valuable in specific situations.
When Testing Is Warranted
Your dermatologist or doctor may recommend hormone testing if:
- Your acne is severe and not responding to standard treatments
- You have signs of androgen excess beyond acne (irregular periods, hirsutism, hair loss)
- Your acne started very early (before age 8) or very late (sudden onset in late teens with no prior history)
- You are a girl with acne concentrated heavily on the jawline and chin combined with menstrual irregularities
What Tests to Expect
If hormonal testing is ordered, common panels include:
- Total and free testosterone: Elevated free testosterone is the most common hormonal finding in females with hormonal acne.
- DHEA-S: Elevated levels suggest adrenal contribution to androgen excess.
- Sex hormone-binding globulin (SHBG): Low SHBG means more free (active) testosterone is available to affect the skin.
- 17-hydroxyprogesterone: Screens for congenital adrenal hyperplasia.
- Fasting insulin and glucose: Screens for insulin resistance, which is associated with PCOS and can drive androgen-related acne.
- LH and FSH: The ratio of these pituitary hormones can suggest PCOS.
- Thyroid panel (TSH, free T4): Rules out thyroid-related skin changes.
Timing matters: For girls, blood work is most accurate when drawn during the early follicular phase (days 1-5 of the cycle), when hormone levels are at baseline.
How to Track Your Breakout Patterns
Identifying your pattern requires consistent observation over time. Here is a practical system that works for most teens.
The Simple Tracking Method
Each evening, spend 30 seconds noting three things:
- New breakouts today? Yes or no. If yes, note the zone (forehead, nose, right cheek, left cheek, chin, jawline, back, chest).
- Type of breakout. Surface whitehead, blackhead, red bump, or deep cyst.
- Relevant factors. Where you are in your menstrual cycle (if applicable), stress level (low/medium/high), any dietary changes, new products used, or events like sports with helmets.
Tools for Tracking
- Period-tracking apps with symptom logging (such as Clue or Flo) allow you to tag skin symptoms alongside cycle data, making it easy to spot correlations after a few months.
- A simple notes app or paper journal works just as well. The key is consistency, not complexity.
- Phone photos taken in the same lighting and angle each day or every few days can reveal patterns that are hard to notice in real time.
What to Look For After 2-3 Months
- Consistent location? If breakouts repeatedly cluster in the same zone, that zone's specific characteristics (androgen receptor density, external contact, product exposure) are likely factors.
- Cyclical timing? If breakouts reliably appear at the same point in your cycle, hormonal fluctuations are clearly involved.
- Stress correlation? If breakouts consistently appear 1-2 weeks after stressful periods, the cortisol-androgen pathway is likely contributing.
- External triggers? If one cheek is always worse, or if forehead acne correlates with specific hair products, you may have identified a non-hormonal trigger you can directly address.
 A simple tracking journal does not need to be complicated. Even basic daily notes can reveal clear patterns after 2-3 months of consistent tracking.
A simple tracking journal does not need to be complicated. Even basic daily notes can reveal clear patterns after 2-3 months of consistent tracking.
Putting It All Together
Your acne is trying to tell you something. Not in the mystical face-mapping sense of "your liver is unhappy," but in a genuinely physiological way. The location, timing, character, and responsiveness of your breakouts carry real diagnostic information.
Here is how to use what you have learned:
If your acne is concentrated on the jawline and chin, hormonal androgen activity is the most likely primary driver. For girls, tracking against your menstrual cycle can confirm this. Treatment approaches that address the hormonal component — rather than just topical antibacterials — are likely to be most effective.
If your acne follows a cyclical monthly pattern, you have strong evidence of hormonal involvement. Bring your tracking data to your dermatologist. This information can directly influence treatment decisions, potentially including hormonal therapies like oral contraceptives or spironolactone for appropriate candidates.
If your acne is widespread across the face, back, and chest, particularly if you are a teenage boy in the peak puberty years, the sheer volume of androgens your body is producing is likely the primary factor. This does not mean treatment is hopeless — it means your dermatologist has a clear picture of what is driving severity.
If your acne is confined to the forehead or T-zone, hormones are a contributing factor (they always are), but product choices, hair care routines, and comedogenic ingredients may be equally or more important to address.
If you notice any signs of hormonal excess beyond acne — irregular periods, excessive hair growth, hair thinning, or rapid weight changes — bring these up with your doctor. These patterns can point to conditions like PCOS that benefit from specific diagnosis and management.
The most important thing you can do right now is start paying attention. Track your breakouts for two to three cycles. Note the where, the when, and the what. That data transforms a frustrating guessing game into an informed conversation with your healthcare provider — and moves you closer to a solution that actually addresses the root cause.
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider for diagnosis and treatment of acne or any medical condition.
How we reviewed this article:
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
- Bhate K, Williams HC. (2013). Epidemiology of acne vulgaris. British Journal of Dermatology.https://pubmed.ncbi.nlm.nih.gov/23210645/
- Zeichner JA, et al. (2017). Emerging issues in adult female acne. Journal of Clinical and Aesthetic Dermatology.https://pubmed.ncbi.nlm.nih.gov/28210380/
- Ju Q, et al. (2017). Sex hormones and acne. Clinics in Dermatology.https://pubmed.ncbi.nlm.nih.gov/28274361/
- Zaenglein AL, et al. (2016). Guidelines of care for acne vulgaris. JAAD.https://pubmed.ncbi.nlm.nih.gov/26897386/
- Lucky AW, et al. (1994). Acne vulgaris in premenarchal girls. Archives of Dermatology.https://pubmed.ncbi.nlm.nih.gov/8002649/
- Thiboutot D. (2004). Acne: Hormonal concepts and therapy. Clinics in Dermatology.https://pubmed.ncbi.nlm.nih.gov/15556720/
- Geller L, et al. (2014). Perimenstrual flare of adult acne. Journal of Clinical and Aesthetic Dermatology.https://pubmed.ncbi.nlm.nih.gov/25489382/
- Preneau S, Dréno B. (2012). Female acne — a different subtype of teenager acne? JEADV.https://pubmed.ncbi.nlm.nih.gov/22329442/
- American Academy of Dermatology. Hormonal acne.https://www.aad.org/public/diseases/acne
- Kim GK, Del Rosso JQ. (2012). Oral spironolactone in post-teenage female patients with acne vulgaris. JCAD.https://pubmed.ncbi.nlm.nih.gov/22468177/
Read This Next

Acne Face Mapping: Does Where You Break Out Tell You Why?

PCOS and Acne in Teens: When Breakouts Signal Something Bigger
If your acne won't respond to normal treatments and comes with irregular periods, it might be PCOS. Here's what teen girls and their parents need to know about diagnosis and treatment.
Read More →
Testosterone and Acne: Why Hormones Drive Most Teen Breakouts
Testosterone gets converted to DHT, which ramps up your oil glands. This is the core reason acne peaks during puberty and why boys tend to get it worse than girls.
Read More →
Inflammatory Acne: Papules, Pustules, and Why Your Skin Hurts
Inflammatory acne is the red, painful kind that actually hurts. Understanding the immune response behind it changes how you treat it and helps you stop making it worse.
Read More →
Comedonal Acne: Why Your Skin Is Bumpy But Not Red (And How to Fix It)
Comedonal acne gives you textured, bumpy skin without the redness of typical pimples. It's frustrating because it doesn't respond to the usual treatments. Here's what actually works.
Read More →