Hormonal Acne in Teenagers: Why It Happens and What Actually Works
Medically reviewed by Dr. Rachel Torres, MD, Pediatric Dermatologist
Written by Teen Acne Solutions Editorial Team — Updated March 16, 2026
Key takeaways
- Hormonal acne is driven by androgens — hormones like testosterone and DHT that surge during puberty and overstimulate oil glands in the skin.
- It looks different in boys vs. girls — boys tend to get more severe, widespread acne, while girls often see cyclical breakouts concentrated on the lower face.
- Topical retinoids and benzoyl peroxide are first-line treatments for most teens, but moderate-to-severe cases may need oral medications.
- Girls have additional options — hormonal treatments like oral contraceptives or spironolactone can target the root androgen-driven cause.
- Most teen hormonal acne improves by the early 20s as hormone levels stabilize, but early treatment helps prevent scarring and emotional distress.
If your teenager is breaking out and nothing seems to help, there is a good chance hormones are the driving force. Hormonal acne is not a sign of poor hygiene or a failed skincare routine — it is a biological process that virtually every adolescent goes through to some degree. Around 85% of teenagers between ages 12 and 24 experience acne, and for most of them, fluctuating hormones are the primary trigger.
Understanding why hormonal acne happens gives you and your teen a genuine advantage. Instead of cycling through random products, you can target the actual cause — and that makes treatment far more effective. Let's break down the science in plain language, look at how hormonal acne shows up differently in boys and girls, and walk through what dermatologists actually recommend.
What Is Hormonal Acne, Exactly?
Hormonal acne is acne that is primarily driven by changes in hormone levels — specifically a group of hormones called androgens. While all acne involves clogged pores, bacteria, and inflammation to some extent, hormonal acne has a distinct underlying engine: your teen's endocrine system is sending signals that cause the oil glands in the skin to go into overdrive.
The term "hormonal acne" is sometimes used to describe adult women's acne that flares around the menstrual cycle. But in reality, the most common form of hormonal acne on the planet is the kind that shows up during puberty. When a dermatologist sees a 13-year-old with new-onset breakouts, the first thing they consider is the hormonal changes of adolescence.
This does not mean hormonal acne is "just part of growing up" and should be left untreated. Moderate-to-severe acne can cause permanent scarring and significant emotional distress. The earlier you address it with the right approach, the better the outcome.
The Puberty-Acne Connection
To understand teen hormonal acne, you need to understand what is happening inside the body during puberty. Here is the chain of events, step by step.
The Role of Androgens
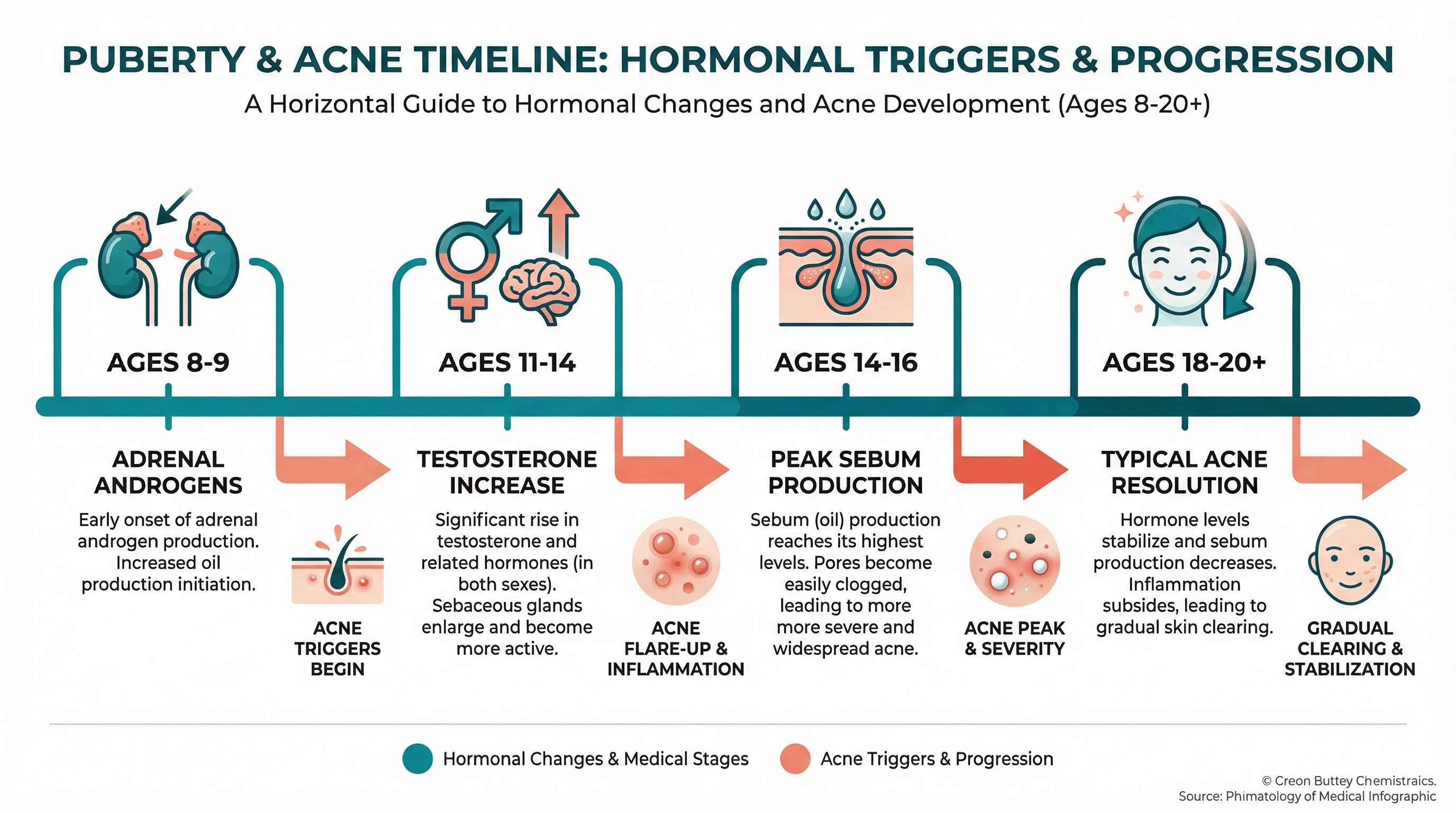
Puberty begins when the hypothalamus and pituitary gland in the brain start signaling the body to produce significantly higher levels of sex hormones. Among these are the androgens — a group that includes testosterone, dehydroepiandrosterone sulfate (DHEA-S), and dihydrotestosterone (DHT).
Both boys and girls produce androgens. Boys produce them primarily in the testes, while girls produce smaller amounts in the ovaries and adrenal glands. During puberty, androgen levels rise dramatically in both sexes, though the increase is much steeper in boys — which is a major reason boys tend to develop more severe acne.
From Androgens to Oil to Breakouts
Here is the critical pathway:
- Androgen levels rise during puberty, sometimes years before other visible signs of adolescence appear. In fact, acne can be one of the very first signs that puberty has begun.
- Androgens stimulate sebaceous (oil) glands. The skin contains thousands of tiny oil-producing glands attached to hair follicles. These glands have androgen receptors on their cell surfaces. When androgens — especially DHT — bind to these receptors, the glands enlarge and start producing far more sebum (oil).
- Excess sebum clogs pores. The increased oil mixes with dead skin cells inside the hair follicle, forming a plug called a microcomedone.
- Bacteria multiply. A bacterium called Cutibacterium acnes (formerly Propionibacterium acnes) thrives in the oily, oxygen-poor environment of a clogged pore.
- Inflammation follows. The immune system responds to the bacterial overgrowth, producing the redness, swelling, and soreness that define inflammatory acne — papules, pustules, nodules, and cysts.
The DHT Factor
Among all the androgens, DHT is the most potent driver of acne. An enzyme called 5-alpha reductase converts testosterone into DHT within the skin itself. DHT is roughly five to ten times more powerful than testosterone at stimulating sebaceous glands. This is why some teens with normal overall testosterone levels can still develop severe acne — their skin may be especially efficient at converting testosterone to DHT, or their sebaceous glands may be particularly sensitive to it.
This enzyme activity varies from person to person, which helps explain why two teenagers going through puberty at the same time can have completely different skin. Genetics play a significant role: if one or both parents had significant acne as teenagers, their child is considerably more likely to experience it as well.
Why It Starts When It Does
Acne often appears between ages 11 and 14 in girls and 12 and 15 in boys, reflecting the typical timing of puberty. However, some children develop acne as early as 8 or 9 — a phenomenon sometimes called prepubertal acne — because adrenal androgens like DHEA-S begin rising even before the full hormonal cascade of puberty kicks in. If your younger child is breaking out, this is likely why, and it is worth mentioning to their pediatrician.
How to Tell If Your Teen's Acne Is Hormonal
Almost all teenage acne has a hormonal component. But certain patterns can help you and your dermatologist determine whether hormones are the primary driver versus other factors like product use, friction, or dietary triggers.
Telltale Signs of Hormonal Acne
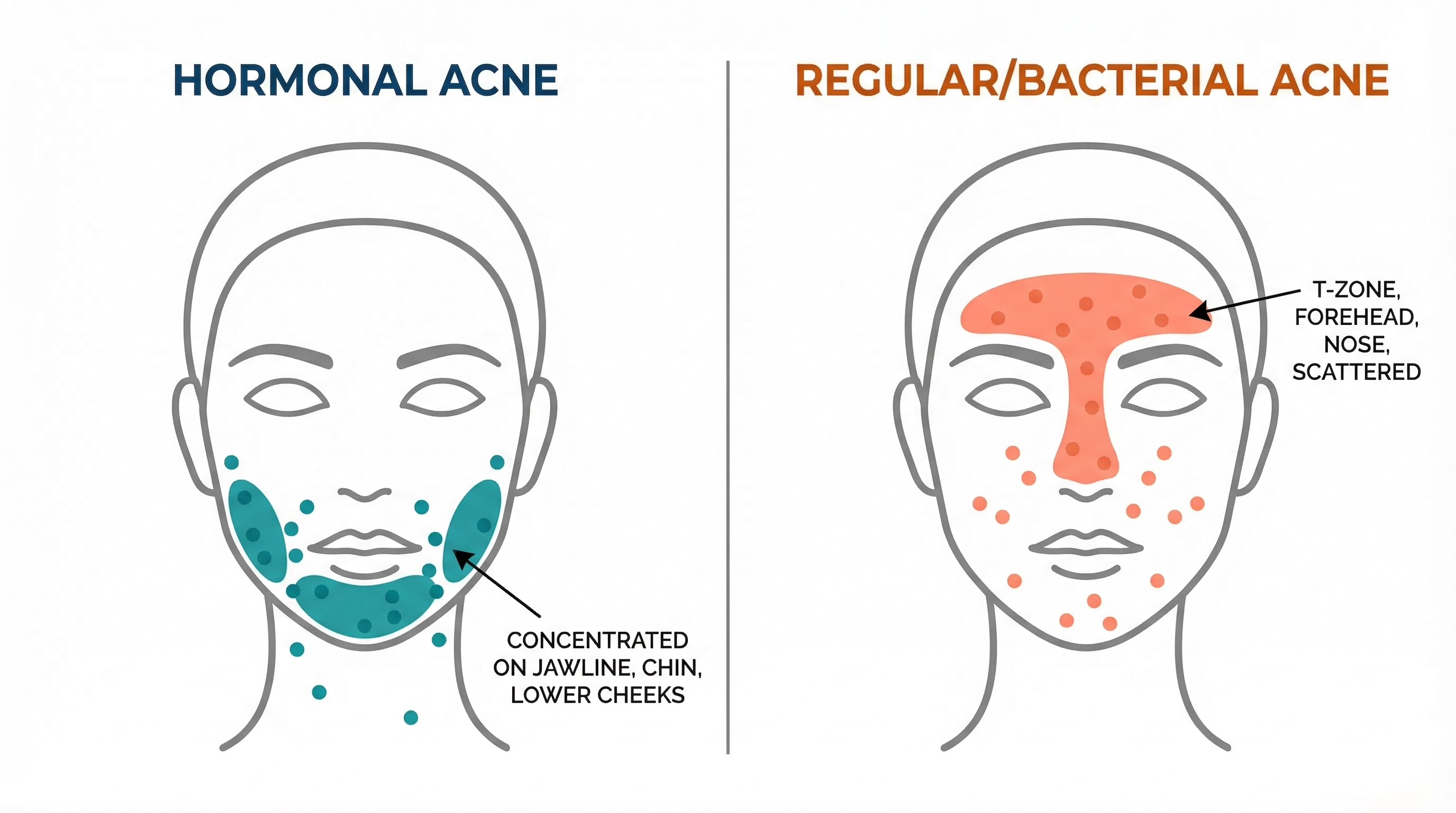
- Location matters. Hormonal acne tends to appear in areas where sebaceous glands are most dense and most responsive to androgens: the T-zone (forehead, nose, chin) in younger teens, and increasingly along the jawline, chin, and lower cheeks as teens get older.
- Deep, painful lesions. Hormonal acne often produces cystic or nodular breakouts — hard, painful bumps under the skin that do not come to a head easily. These are driven by intense inflammation deep in the follicle.
- Oily skin. If your teen's skin has become noticeably oilier over the past year or two, that is the androgens at work.
- Timing with puberty. Acne that started around the same time as other signs of puberty (growth spurts, body hair, voice changes, breast development) is almost certainly hormonal.
- Resistance to basic treatments. Truly hormonal acne often does not clear fully with cleansing and over-the-counter spot treatments alone, because the underlying cause is systemic.

Hormonal Acne in Girls vs. Boys
The hormonal acne experience can differ quite a bit depending on sex.
In boys:
- Acne tends to be more severe overall because of higher androgen levels
- It commonly affects the forehead, cheeks, back, and chest in addition to the face
- Nodular and cystic acne is more common
- It often peaks between ages 16 and 19
- Boys are more likely to need isotretinoin (Accutane) for severe cases
In girls:
- Acne is often milder but more persistent
- It frequently concentrates on the lower face — jawline, chin, and around the mouth
- Many girls notice breakouts worsening in the week before their period, as progesterone rises and estrogen drops, shifting the androgen-to-estrogen ratio in favor of androgens
- It may persist or even begin after puberty, extending well into the 20s
- Girls have additional treatment options (hormonal therapies) that boys do not
Research published in the Archives of Dermatology has documented that up to 63% of women with acne experience premenstrual flares, making cyclical breakouts one of the most reliable indicators of hormonal acne in teenage girls and young women.
Treatment Options That Actually Work
Treating hormonal acne in teenagers means addressing both the immediate breakouts and the underlying hormonal triggers. Here is how dermatologists typically approach it, from first-line treatments to more advanced options.
First-Line Topical Treatments
For mild-to-moderate hormonal acne, topical treatments are the starting point. These work on the skin's surface and within the pores to reduce oil, unclog follicles, and kill bacteria.
Topical retinoids are considered the backbone of acne treatment by every major dermatology guideline. Adapalene (Differin) is available over the counter at 0.1% strength, while stronger retinoids like tretinoin and tazarotene require a prescription. Retinoids work by:
- Normalizing the way skin cells shed inside the follicle, preventing clogs
- Reducing microcomedone formation (the earliest stage of a pimple)
- Having mild anti-inflammatory properties
Retinoids take time — typically 8 to 12 weeks — to show meaningful results. Skin often gets slightly worse before it gets better, a phase sometimes called "purging." This is normal and is a sign the medication is working.
Benzoyl peroxide (2.5% to 5%) kills C. acnes bacteria and has mild pore-unclogging properties. Unlike antibiotics, bacteria do not develop resistance to benzoyl peroxide, making it safe for long-term use. It pairs extremely well with a retinoid — one in the morning, one at night.
Combination approach. Dermatologists almost always recommend using a retinoid and benzoyl peroxide together rather than either alone. Studies consistently show that combination therapy clears acne faster and more completely.
Oral Medications for Moderate-to-Severe Cases
When topical treatments alone are not enough — especially when acne is widespread, deeply inflammatory, or causing scarring — oral medications come into play.
Oral antibiotics like doxycycline or minocycline reduce both bacteria and inflammation. They work relatively quickly (improvement often visible within 4 to 6 weeks) but should be used for the shortest effective duration — ideally 3 to 4 months — to minimize the risk of antibiotic resistance. They are always used alongside topical retinoids and benzoyl peroxide, never alone.
Isotretinoin (Accutane) is reserved for severe, scarring, or treatment-resistant acne. It is the only medication that addresses all four causes of acne simultaneously: oil production, pore clogging, bacterial growth, and inflammation. About 85% of patients see significant or complete clearing after one course (typically 5 to 7 months). It carries real side effects and requires careful monitoring, but for teens with severe hormonal acne, it can be genuinely life-changing.

Hormonal Treatments (Girls Only)
Because androgens are the root driver of hormonal acne, treatments that modulate androgen levels or block their effects can be highly effective. These options are available for girls and young women but are not used in boys.
Combined oral contraceptives (birth control pills) that contain both estrogen and a progestin can reduce acne by:
- Increasing sex hormone-binding globulin (SHBG), a protein in the blood that binds to free testosterone and makes it inactive
- Reducing the ovaries' production of androgens
- Lowering circulating levels of free testosterone and DHT
The FDA has specifically approved several oral contraceptives for acne treatment, including those containing norgestimate, norethindrone acetate/ethinyl estradiol, and drospirenone. It typically takes 2 to 3 months to see improvement, with full results by 6 months.
Spironolactone is a medication originally developed for blood pressure that also blocks androgen receptors and reduces androgen production. Dermatologists frequently prescribe it off-label for teenage girls (typically age 15+) with hormonal acne that has not responded to standard treatments. Doses typically range from 50 to 100 mg daily. Studies show it reduces acne severity by 50 to 100% in most patients. It is not appropriate for boys because of its anti-androgen effects.
A note for parents: Suggesting birth control pills for acne treatment can feel complicated. It may help to know that dermatologists prescribe these specifically for their effect on skin — the contraceptive function is secondary. Having an open, straightforward conversation with your teen and their doctor can help everyone feel comfortable with the treatment plan.
Building a Complete Treatment Plan
For most teens with hormonal acne, an effective plan looks something like this:
- Gentle cleanser — twice daily, fragrance-free, non-comedogenic
- Topical retinoid — applied at night (start every other night to build tolerance)
- Benzoyl peroxide — applied in the morning, or used as a short-contact wash
- Oil-free moisturizer and sunscreen — daily, since both retinoids and benzoyl peroxide increase sun sensitivity
- Oral medication if needed — antibiotics for a short course, hormonal options for girls, or isotretinoin for severe cases
Patience is essential. Most acne treatments take a full 8 to 12 weeks to show real results. Switching products every two weeks because "nothing is working" is one of the most common mistakes teens make. Set expectations early: improvement is gradual, not overnight.
Lifestyle Factors That Make a Real Difference
Hormonal acne cannot be cured by lifestyle changes alone — the hormonal driver is too powerful. But certain habits can meaningfully reduce breakout severity and help treatments work better.
Diet
The relationship between diet and acne has been debated for decades, but recent research has clarified a few connections:
- High-glycemic foods (white bread, sugary cereals, candy, soda) cause rapid spikes in blood sugar and insulin. Elevated insulin increases levels of insulin-like growth factor 1 (IGF-1), which in turn stimulates androgen production and sebum output. Studies have found that low-glycemic diets are associated with reduced acne severity.
- Dairy — particularly skim milk — has been linked to acne in several large observational studies. The mechanism is not fully established, but may involve naturally occurring hormones and bioactive molecules in cow's milk that influence human androgen pathways.
- There is no need for extreme elimination diets. A balanced diet that emphasizes whole grains, vegetables, lean proteins, and healthy fats while limiting processed sugars and excessive dairy is reasonable, evidence-based advice.
Stress
Stress does not directly cause hormonal acne, but it can make it worse. The adrenal glands produce cortisol and DHEA-S in response to stress, and DHEA-S is an androgen precursor. Chronic stress — whether from school pressure, social dynamics, or the emotional toll of having acne itself — can keep androgen levels elevated and worsen breakouts.
Encouraging healthy stress management is genuinely helpful: regular physical activity, adequate sleep (8 to 10 hours for teens), and maintaining social connections all contribute. Teens dealing with acne-related anxiety or depression should be connected with a mental health professional — this is more common than many parents realize.
Sleep and Exercise
Both are important but often overlooked:
- Sleep is when the body regulates many hormones, including cortisol and growth hormone. Chronic sleep deprivation — extremely common in teenagers — can disrupt this regulation and contribute to breakouts.
- Exercise helps regulate insulin sensitivity and reduces stress hormones. The sweat itself does not cause acne, but leaving sweat mixed with oil and bacteria on the skin for hours can. A quick rinse or gentle cleanse after workouts helps.
What Does NOT Cause Hormonal Acne
It is worth clearing up some persistent myths:
- Dirty skin does not cause acne. Over-washing can actually worsen it by stripping the skin barrier and triggering compensatory oil production.
- Chocolate, greasy food, and pizza have not been shown to directly cause acne (though the high-glycemic and dairy components of some of these foods may contribute).
- Touching your face does not cause hormonal acne, though it can introduce bacteria and worsen existing breakouts.
The Emotional Side of Hormonal Acne
We would be doing a disservice not to talk about this. Hormonal acne shows up during one of the most socially sensitive periods of a person's life. Research consistently shows that acne — even mild acne — is associated with higher rates of anxiety, depression, low self-esteem, and social withdrawal in teenagers.
If your teen is withdrawing from activities, seems unusually down, avoids being photographed, or makes comments about feeling ugly or hopeless, please take those signals seriously. Acne is a medical condition, not a cosmetic inconvenience. Seeking treatment is not vanity — it is healthcare.
For teens reading this: what you are going through is real, it is not your fault, and it is treatable. You are not alone. Talk to a parent, school counselor, or doctor. You deserve support.
When Does It Get Better?
This is the question every teenager (and parent) wants answered.
The good news: for the majority of people, hormonal acne improves significantly as puberty winds down and hormone levels stabilize. Here is a general timeline:
- Boys: Acne often peaks between ages 16 and 19 and begins to improve in the late teens to early 20s. By the mid-20s, most men see substantial clearing.
- Girls: The trajectory is less predictable. Many girls see improvement by their late teens, but a significant percentage — estimated at 12 to 22% of women — continue to experience hormonal acne well into their 20s and even 30s, particularly around the menstrual cycle.
The not-so-good news: waiting it out without treatment is rarely the best strategy. Untreated moderate-to-severe acne can cause:
- Permanent scarring (both pitted and raised)
- Post-inflammatory hyperpigmentation (dark marks that can last months to years, especially in darker skin tones)
- Psychological harm that can have lasting effects on self-esteem and social development
Early, appropriate treatment shortens the duration, reduces scarring risk, and helps teens feel better about themselves during a critical developmental period.
When to See a Dermatologist
Not all teen acne requires a specialist, but hormonal acne often does. Consider making an appointment if:
- Over-the-counter treatments have not shown improvement after 8 to 12 weeks of consistent use
- Your teen has painful, deep cysts or nodules
- Acne is leaving scars or dark marks
- Breakouts are widespread (face, chest, and back)
- Your teen is emotionally struggling because of their skin
- You suspect a hormonal imbalance beyond normal puberty (signs might include very early puberty, irregular periods, or excessive body hair in girls)
A dermatologist can evaluate whether standard topical therapy is sufficient or whether oral medications, hormonal treatments, or isotretinoin should be considered. They can also check for underlying conditions like polycystic ovary syndrome (PCOS) in girls, which can cause persistent hormonal acne alongside other symptoms.
Bottom Line
Hormonal acne in teenagers is overwhelmingly common, biologically driven, and — most importantly — treatable. It happens because puberty floods the body with androgens that overstimulate the skin's oil glands, creating the perfect conditions for clogged pores, bacterial growth, and inflammation.
The single most important thing you can do is take it seriously and start treatment early. A combination of topical retinoids and benzoyl peroxide handles most mild-to-moderate cases. For more stubborn breakouts, oral antibiotics, hormonal therapies (for girls), or isotretinoin offer powerful solutions. Pair medical treatment with a simple, consistent skincare routine, a balanced diet, good sleep, and stress management — and give it time to work.
Your teen did not choose this, and they cannot wash it away. But with the right approach, hormonal acne is one of the most manageable conditions in dermatology. Talk to a dermatologist, build a plan, and stick with it. Clearer skin — and more confidence — are within reach.
How we reviewed this article:
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-973https://pubmed.ncbi.nlm.nih.gov/26897386/
- Zouboulis CC, Bettoli V. Management of severe acne. Br J Dermatol. 2015;172 Suppl 1:27-36https://pubmed.ncbi.nlm.nih.gov/25597636/
- Tan JK, Bhate K. A global perspective on the epidemiology of acne. Br J Dermatol. 2015;172 Suppl 1:3-12https://pubmed.ncbi.nlm.nih.gov/25597339/
- Leyden J, Stein-Gold L, Weiss J. Why topical retinoids are mainstay of therapy for acne. Dermatol Ther (Heidelb). 2017;7(3):293-304https://pubmed.ncbi.nlm.nih.gov/28585191/
- Thiboutot D, Gollnick H, Bettoli V, et al. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009;60(5 Suppl):S1-S50https://pubmed.ncbi.nlm.nih.gov/19376456/
- Elsaie ML. Hormonal treatment of acne vulgaris: an update. Clin Cosmet Investig Dermatol. 2016;9:241-248https://pubmed.ncbi.nlm.nih.gov/27621661/
- American Academy of Dermatology. Acne: Who Gets and Causes. AAD. 2024https://www.aad.org/public/diseases/acne/causes/acne-causes
- Lucky AW. Quantitative documentation of a premenstrual flare of facial acne in adult women. Arch Dermatol. 2004;140(4):423-424https://pubmed.ncbi.nlm.nih.gov/15096370/
- Knutsen-Larson S, Dawson AL, Dunnick CA, Dellavalle RP. Acne vulgaris: pathogenesis, treatment, and needs assessment. Dermatol Clin. 2012;30(1):99-106https://pubmed.ncbi.nlm.nih.gov/22117871/
- Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol. 2013;168(3):474-485https://pubmed.ncbi.nlm.nih.gov/23210645/
- Melnik BC. Role of insulin, insulin-like growth factor-1, hyperglycaemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009;18(10):833-841https://pubmed.ncbi.nlm.nih.gov/19709092/
Read This Next

The Acne Glossary: Every Term You'll Encounter, Explained Simply
From adapalene to zinc, every acne and skincare term you'll run into, defined in plain language without the medical jargon.
Read More →
Micellar Water for Acne-Prone Skin: Gentle Cleanser or Lazy Shortcut?
Micellar water is fine for light cleansing days but won't remove sunscreen properly. Here's when to use it, when to skip it, and whether you need to rinse.
Read More →
How Seasonal Changes Affect Your Acne (And When to Switch Products)

Going to College with Acne: Preparing Your Skincare for Dorm Life
